Introduction
The ability to perform percutaneous or limited incision access for deployment of stent grafts defines endovascular surgery. This summary will highlight endovascular access methods as well as common complications associated with the procedures.
Choice of Approach
The most common percutaneous access sites are the femoral, radial, and brachial arteries. When choosing which site to access the vascular tree, one must not only consider the intended procedure but also the size of the sheath and distance to the pathology. The goal for percutaneous access is to create the smallest incision, that provides safe and effective entry, without creating vascular trauma. Sheaths up to 10 Fr (3.3 mm) can be safely placed percutaneously. Larger sheaths require a cut down to ensure vascular hemostasis and minimize traumatic injury. If the physician is not adaptive to utilizing alternative access sites, then the procedure will be compromised.
 |
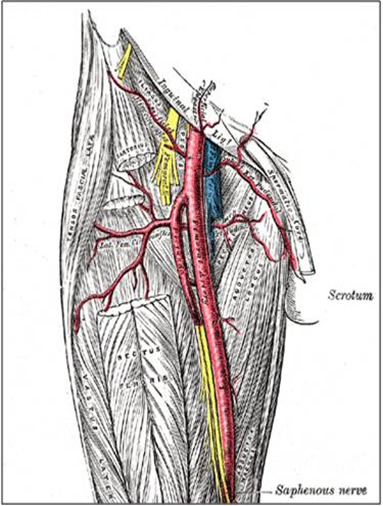
| Figure 1: Access below the inguinal ligament. |
Percutaneous Retrograde Femoral Artery Access
Most right handed physicians will prefer the patient’s right groin for femoral access, although both groins should be prepped in case of inaccessibility. After the pulse is identified, the inguinal ligament is found by tracing a line between the anterior iliac spine and the pubic tubercle. Often, especially in obese individuals, the inguinal crease is inferior to this landmark. Access should be made below the inguinal ligament corresponding to the common femoral artery (Figure 1). One will find that if access is made too high, corresponding with the external iliac artery, hemostasis is difficult to achieve with manual pressure. In this case hemorrhage can occur after removal of devices and a retroperitoneal hematoma can develop. This is often insidious in onset. In addition, the risk of pseudoaneurysm formation is higher in an external iliac stick, again because direct manual pressure cannot be applied this superiorly.
 |
| Figure 2: Cartoon depecting radiologic access. |
A properly equipped endovascular suite will allow fluoroscopic imaging of the groin to identify all anatomic landmarks. In addition to surface landmarks, most physicians use the medial half of the femoral head to guide femoral artery access (Figure 2). This ensures common femoral artery entry and avoids the complications of a higher stick. It is also useful in the pulseless femoral artery.
Most vascular access kits include an 18 gauge straight angiographic entry needle. This is inserted using the dominant hand at a 45-degree angle while using the non-dominant hand for guidance. After pulsatile bright red bleeding is occurred, a wire exchange is performed using the Seldinger technique. In instances where the vessel may be small, calcified, or tortuous, a smaller access needle may be desirable. A micro-puncture kit (Cook, Inc., Bloomington, IN) exists which includes a 21 gauge needle for initial access. A floppy tipped 0.018 inch guidewire is then threaded, followed by removal of the needle. A 4 Fr short catheter with 3 Fr inner dilator is placed over the existing wire, followed by removal of the dilator and wire. Then, an appropriately sized wire (0.035 in) can be placed through the 4 Fr catheter with subsequent upsizing to an appropriately sized sheath.
 |
| Figure 3: Anatomic representation of the femoral vessels. |
Open Femoral Artery Access
When utilizing a sheath larger than 10 Fr, open femoral artery access is preferred to ensure hemostasis. With the patient supine, the pulse is palpated just below the inguinal ligament. Either a longitudinal, horizontal, or oblique incision, about 2-3 cm in length, is made. Electrocautery is used to dissect the subcutaneous tissue down to the level of the fascia. A self-retaining retractor aids in exposure. After the fascia has been cleared, sharp dissection is used to expose the artery, which is lateral to the femoral vein (Figure 3). If the intended sheath is small, a simple purse-string suture placed on the anterior wall of the vessel may suffice to ensure post-operative hemostasis. However, with larger sheaths, gaining proximal and distal control of the vessel is advised so that the artery can be closed in an open fashion at the conclusion of the case. This method will help prevent stenosis associated with the purse-string closure technique. With the vessel exposed, an 18 gauge needle is directly inserted into the anterior wall of the artery. The Seldinger technique is then used to upsize to the intended sheath.
 |
| Figure 4: So called "iliac-on-a-stick." |
A few of the complications using larger sheaths include: intimal disruption, perforation of the proximal arterial tree, and avulsion of the iliac artery (the so-called “iliac-on-a-stick”) (Figure 4). Arteriography should be performed after removal of the sheath to investigate for any leaks. These can be remedied using covered stents or direct exposure and repair. Bypass grafts may be necessary if a large defect was created. In any event, one must retain wire access across the injury. This allows quick placement of an occluding balloon proximal to the injury, minimizing hemorrhage, and allowing time for open iliac cut-down and repair. If, after removal of the sheath, there is any concern about stenosis from the previously placed purse-string suture, an open repair of the vessel should be performed. After the placement of proximal and distal vascular clamps, the defect is opened using vascular scissors and all debris is cleaned. Any focal dissections or flaps should be removed or tacked to the vessel wall using 6-0 polypropylene suture. The vessel can then be closed using interrupted sutures under direct visualization. The distal clamp is removed before the last suture is tied to allow de-airing. An immediate check of distal pulses should be performed after release of all clamps to ensure good flow. If there is any compromise of flow, the closure should be interrogated.
Proximal Access
Access to the brachial or radial arteries carries not only a higher risk of complications, but the complications are generally more severe than those associated with femoral access. The arteries of the upper extremity have an enveloping fascial sheath. Therefore when a hematoma does occur, brachial plexopathies are more common. In addition, upper extremity vessels tend to spasm more frequently during manipulation, making access more challenging. Brachial access carries the added risk of distal ischemia and embolization over radial access. Although sheaths up to 6 or 7 Fr may be percutaneously placed in either vessel, radial access should be preferred over brachial because of a lower complication profile. Open access should be used for larger sheaths or on smaller patients.
The left brachial artery is preferred over the right so as to avoid the origin of the right common carotid artery. The arm is abducted on an arm board with the arm circumferentially prepped. The artery is palpated just proximal to the antecubital fossa where the biceps muscle thins out to its tendinous insertion. A 21 gauge micropuncture kit is preferred to the 18 gauge due to the smaller size of the vessel. Catheter-over-wire exchange can then be performed to the desired sheath. Radial artery access is performed similarly to any arterial catheter placement. The artery is palpated at the lateral wrist and a 21 or 23 gauge needle is used to enter the vessel. A catheter-over-wire exchange is then performed. Sheaths up to 6 Fr can be placed with relative safety. Long sheaths can help deal with the inherent vasospasm.
Brachial and radial access techniques allow the utilization of angiographic catheters to assist with proximal deployment of thoracic stent grafts. They allow for easy identification of the left subclavian artery, and angiography can be performed to avoid coverage with the proximal end of a thoracic stent. When coverage of the left subclavian artery is required for an adequate proximal landing zone, subclavian to carotid bypassing is often necessary. The radial or brachial access can therefore accommodate subclavian artery coil embolization to minimize the risk of Type II endoleaks.



