|
 |
|
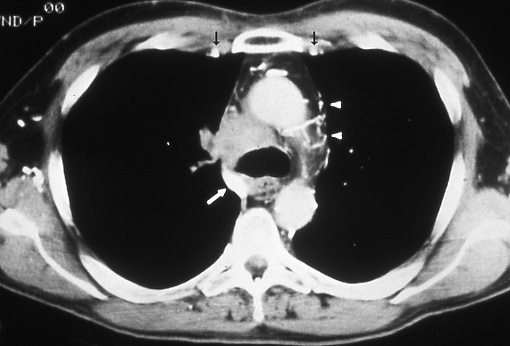
Fig.
53: Computed
tomographic scan of the
chest shows a large mass
in the right paratracheal
area obstructing the
superior vena cava. The
azygous vein (white arrow)
is also obstructed and
multiple small vessels
are seen on the left
side of the mediastinum
(white arrowheads); the
internal mammary veins
are also prominent (black
arrows), T4 N2 M0, stage
IIIB. |
|
|
Involvement of the Vertebral Body
In most
patients with superior sulcus or Pancoast's
tumors with clinical evidence
of vertebral body invasion this extension
of the disease indicates unresectability
and a poor prognosis. There are reports
of patients who have undergone successful
resection for tumors with localized invasion
of a specific area of the vertebral body
who have a better prognosis than that
anticipated for patients with unresectable
disease.
There are investigational surgical programs,
usually multidisciplinary efforts undertaken
by thoracic and neurosurgeons, that address
removal of part or all of the vertebra.
Although a few patients may be found
at operation to have resectable tumor invading
the vertebral body, clinical evidence
of
this extent of disease is generally associated
with non-surgical treatment options and
a prognosis consistent
with the T4 category.
A tumor arising in the superior sulcus
of the lung with evidence for a true Pancoast's
syndrome,
that is, a Horner's syndrome and brachial
plexus involvement, should
be classified T4, whether or not vertebral body invasion is present.
|