
Introduction
The first description of a direct communication between the left ventricle and the right atrium was reported by Buhl in 1857 [1]. The first successful closure of such a defect was first reported by Kirby (using hypothermia and inflow occlusion) at the Hospital of the University of Pennsylvania in 1956 [2]. The first successful series of patients operated on with a left ventricular-to-right atrial shunt was reported by Frank Gerbode, a noted surgeon at Stanford University [3]. Gerbode described two routes for blood to travel from the left ventricle to the right atrium, as shown in Figure 1.
 |
 |  |
| Figure 2 | Figure 3 |
 |  |
| Figure 4 | Figure 5 |
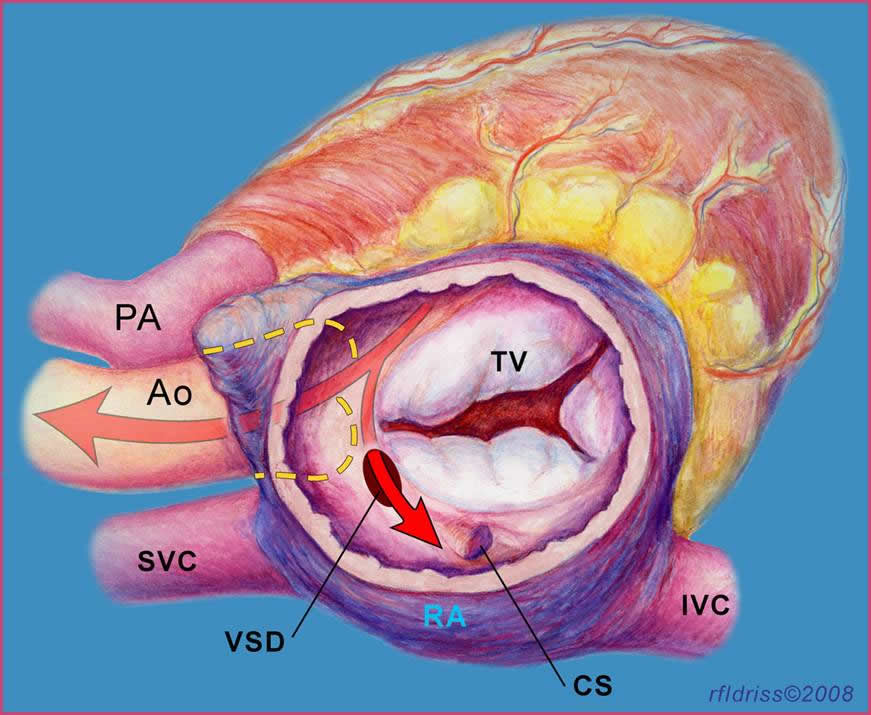
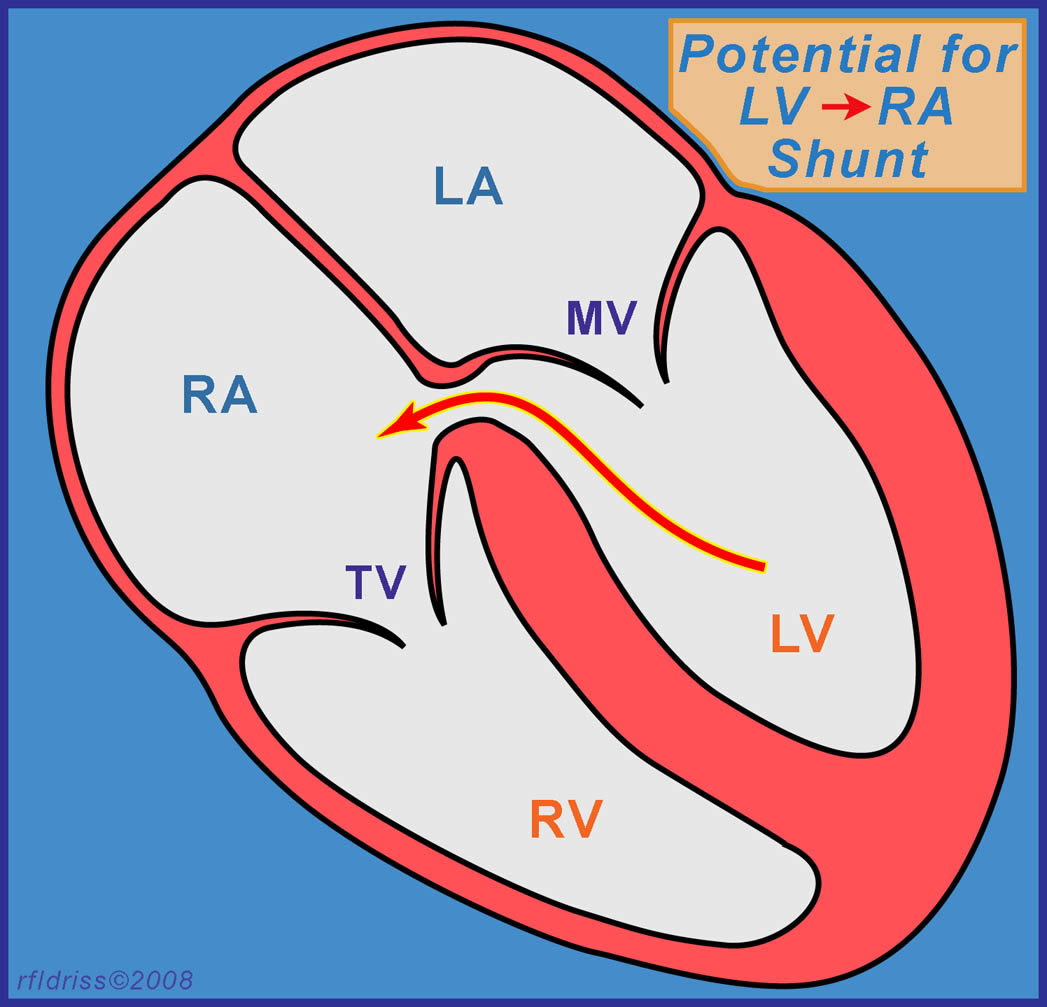
The definition of a Gerbode defect, according to the STS Congenital Heart Nomenclature and Database Project [4], is a true left ventricular-to-right atrial communication. The anatomy of this defect is shown in Figure 2. The blood in the left ventricle goes through the small area of the membranous septum where there is the potential for a left ventricular-to-right atrial shunt as shown in a lateral view in Figure 3. This communication is above the tricuspid valve [5].
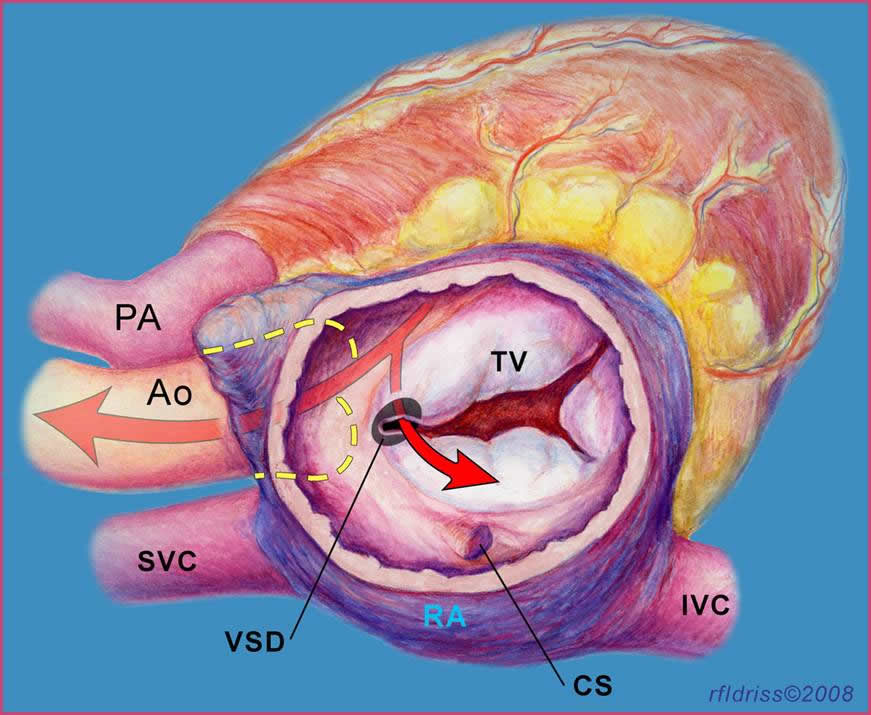
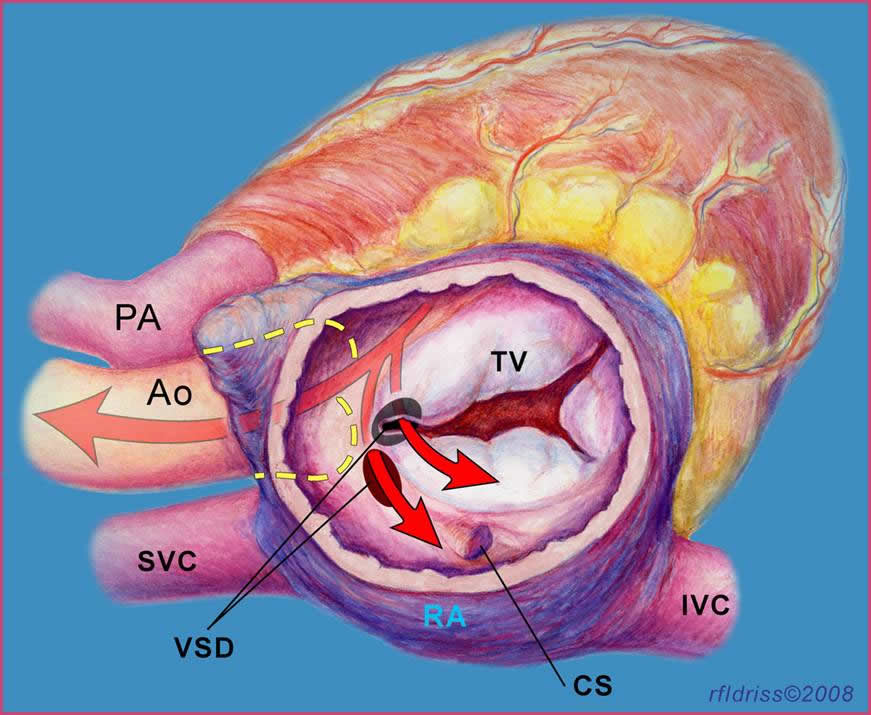
Figure 4 demonstrates the more common, indirect, type of communication where the flow of blood is from the left ventricle through a ventricular septal defect into the right ventricle and then through a defect in the tricuspid valve into the right atrium. The source of this communication occurs below the tricuspid valve [5]. We excluded patients with this type of indirect left ventricular-to-right atrial shunt from our analysis. This series reports only the direct left ventricular-to-right atrial communication. Figure 5 illustrates both defects.
Patient Population
Six patients (2 male, 4 female) underwent closure of a direct congenital Gerbode-type ventriculo-atrial defect between the years 1990 and 2008 at Children’s Memorial Hospital. Three of these patients had congestive heart failure, 2 had failure to thrive, and 2 had exercise intolerance. The median age at time of repair was 1.6 years; age range was 0.4 to 19 years. The size of the ventriculo-atrial defect ranged from 4 to 8 mm, with a mean size of 6.2 ± 2 mm. All patients in this series had an opening on the atrial aspect of the hinge of the tricuspid valve. Given the rarity of this anomaly, it is interesting that most of these patients had associated cardiovascular anomalies. One patient had a right aortic arch, one patient had a patent ductus arteriosus, three patients had a left superior vena cava, two patients had an anomalous left hepatic vein. The left hepatic vein in one patient drained directly to the right atrium, and in another patient drained directly to the coronary sinus.
Diagnostic Technique
 |  |
| Figure 6 | Figure 7 |
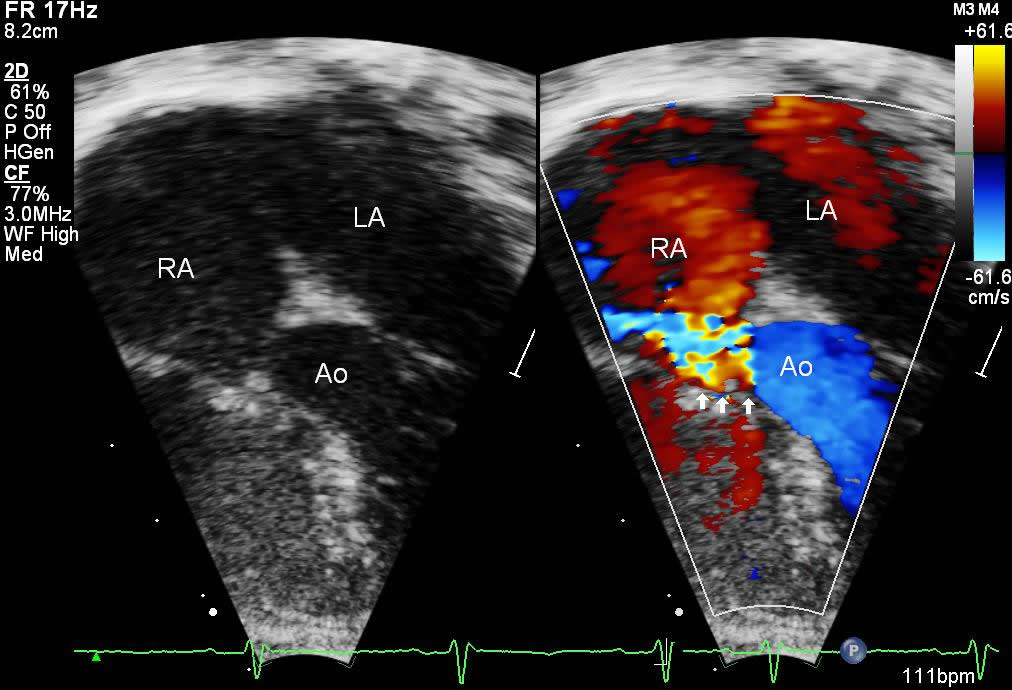
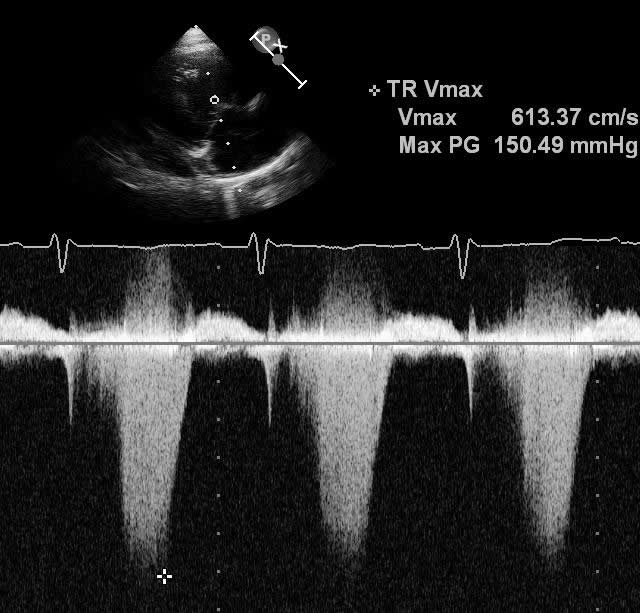
All patients were diagnosed with echocardiography. Figure 6 shows a 4-chamber view where the color Doppler jet travels from the left ventricle into the right atrium. Figure 7 demonstrates the Doppler envelope. The maximum peak instantaneous gradient in this patient was 150 mm Hg. This high Doppler gradient is one of the hallmarks of the Gerbode ventriculo-atrial defect because of the difference between the left ventricular systolic pressure and the low right atrial pressure. The echocardiogram gradient ranged from 65 to 150 mm Hg, with a mean echo gradient of 95 mm Hg. Echocardiography confirmed a dilated right atrium in all patients.
Surgical Technique
All patients were repaired via median sternotomy using cardiopulmonary bypass, aortic cross clamp, cold blood cardioplegia, and patch closure. The mean cardiopulmonary bypass time was 88.6 ± 11.5 minutes. The mean aortic cross-clamp time was 54.4 ± 7.7 minutes.
 |  |
| Figure 8 | Figure 9 |
 |  |
| Figure 10 | Figure 11 |
 |  |
| Figure 12 | Figure 13 |
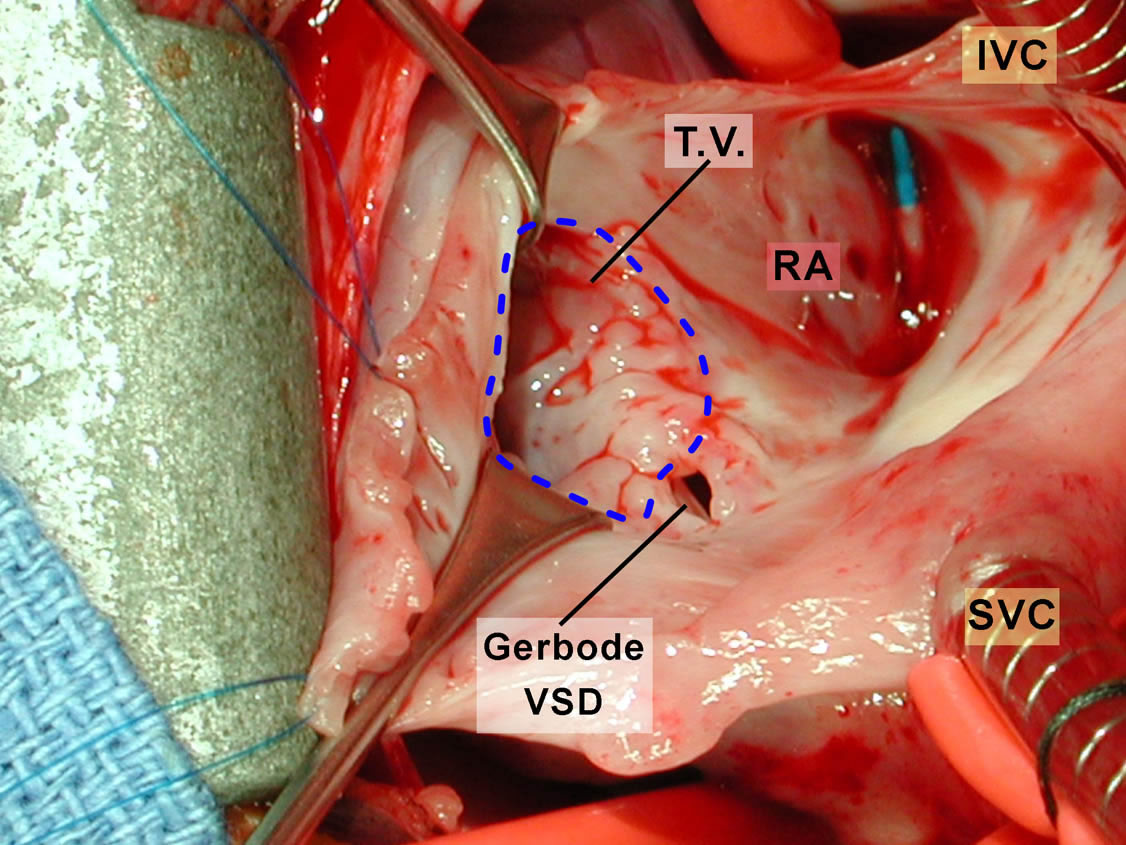
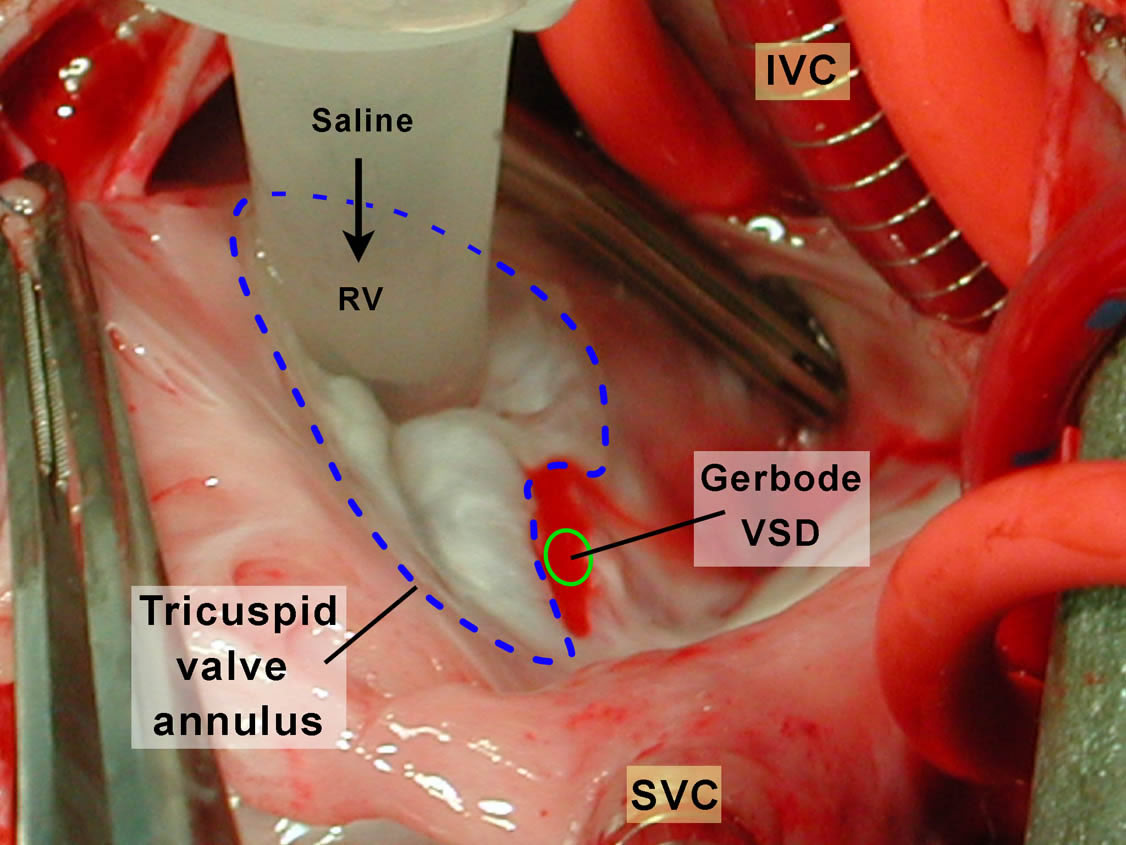
Figure 8 shows the view of the open right atrium taken from the head of the table. The superior vena cava (SVC) and inferior vena cava (IVC) are identified. There is a catheter tip in the mid-portion of the right atrium. The tricuspid valve has been outlined with a dotted blue line. The Gerbode ventriculo-atrial defect is indicated.
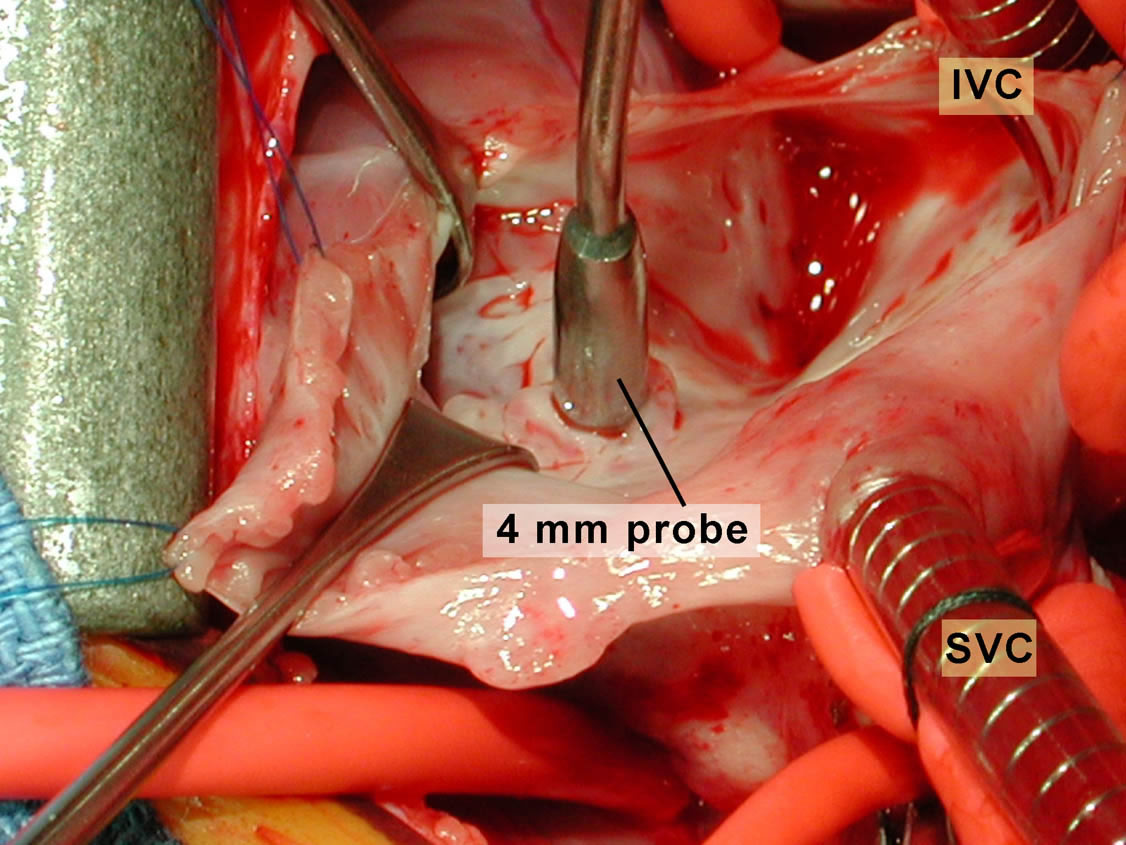
In Figure 9, a 4-mm probe is being shown passed across the ventriculo-atrial defect.
In Figure 10, the surgeon has insufflated the right ventricle with cold saline; the tricuspid valve is seen to be competent. There is no saline coming out of the Gerbode defect, indicating no communication between the right ventricle and the anatomic channel between the left ventricle and the right atrium. There is only a small amount of blood coming out of the Gerbode defect (green circle).
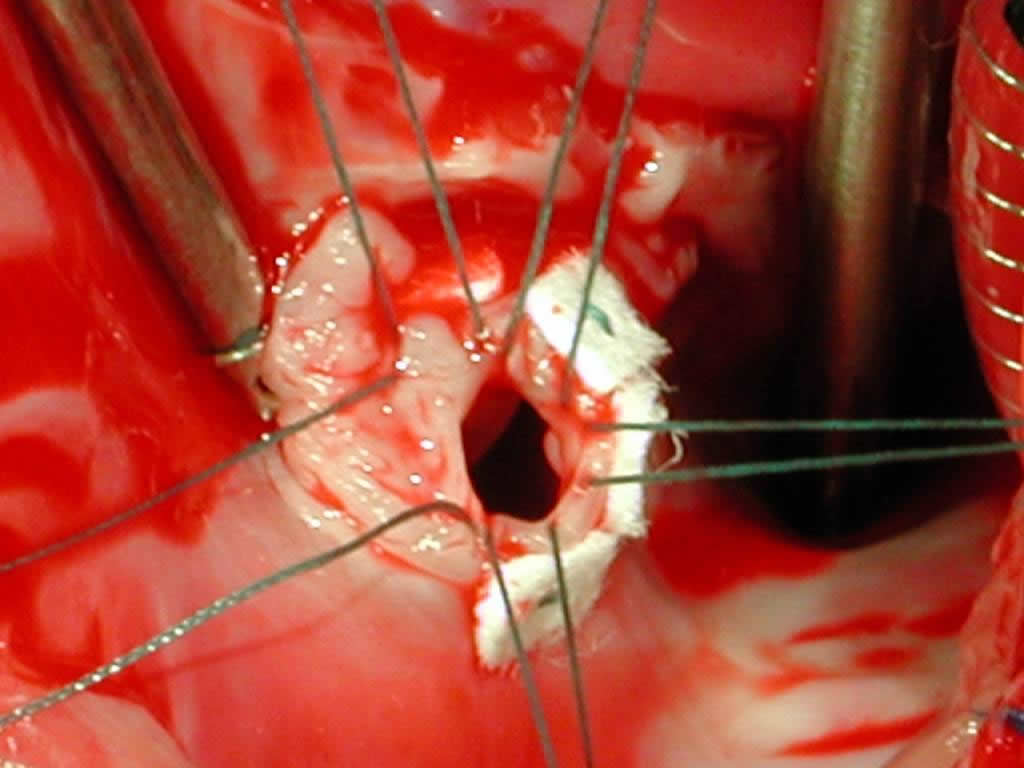
Figure 11 shows the placement of 5 pledget-supported Ticron sutures around the circumference of the ventriculo-atrial defect.
Figure 12 shows a 0.4-mm thickness Gore-Tex® cardiovascular patch in which sutures have been placed, lowered into the field.
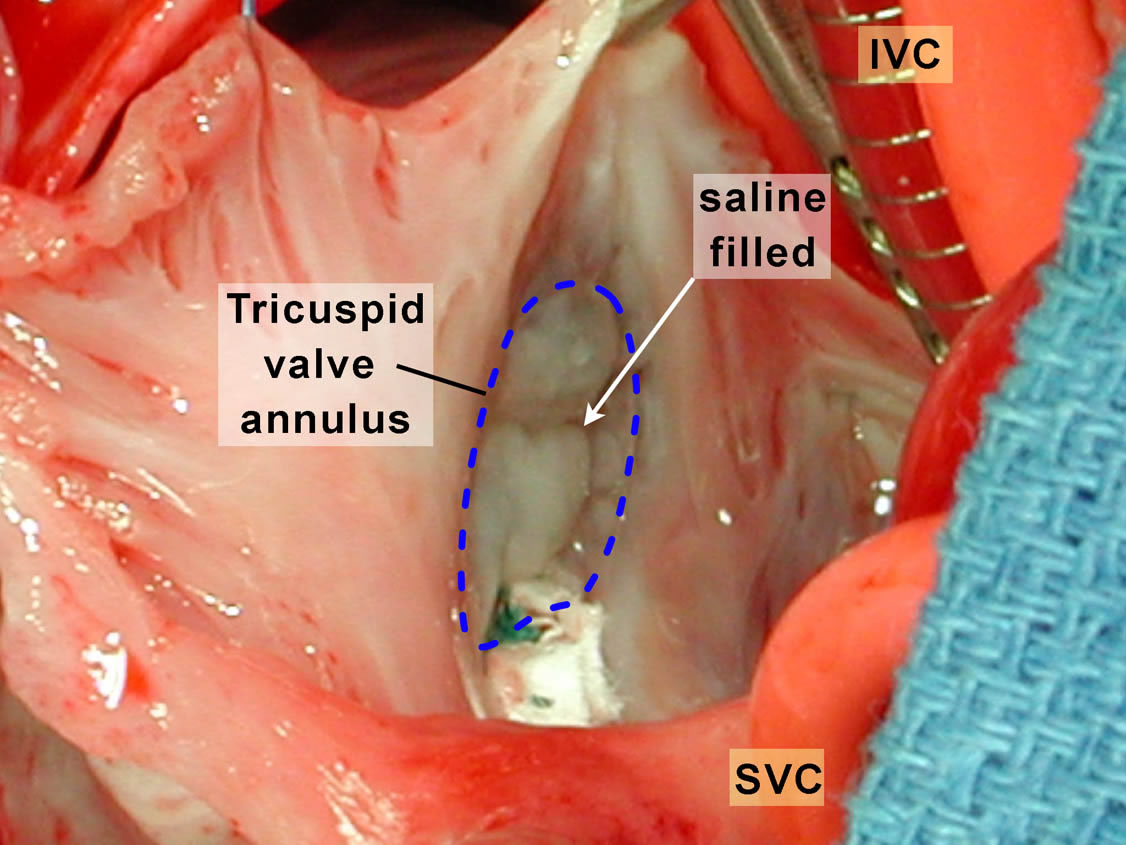
Figure 13 shows the completed repair with the tricuspid valve again filled with saline and demonstrating that the tricuspid valve is competent.
Tips & Pitfalls
- Transesophageal echocardiography (TEE) is helpful to sort out whether this is a direct or indirect left ventricular-to-right atrial shunt. If there is tricuspid valve insufficiency, TEE is helpful to assess the repair.
- Although the defect may in some cases be anatomically small, in all cases we used a patch to prevent recurrence.
Results
In this series of 6 patients with a true direct Gerbode ventriculo-atrial defect, there was no operative or late mortality. Mean postoperative length of stay was 4 days. All patients were in normal sinus rhythm. There were no patients with residual ventriculo-atrial shunting and no patients required a reoperation. Echocardiogram demonstrated at most trivial tricuspid valve regurgitation.
Discussion
The Gerbode ventriculo-atrial defect is a very rare congenital anomaly [6]. We have had 6 of these defects at our institution in the past 19 years. In this time period, we have repaired over 400 isolated perimembranous, muscular, and conal ventricular septal defects. A Gerbode defect should be suspected on echocardiogram when there is an unusually dilated right atrium. The other sine qua non of the Gerbode defect is the high Doppler gradient between the left ventricle and the right atrium. The mean gradient in our series was 95 mm Hg. We recommend closure of essentially all Gerbode defects. In our experience, and surveying other pediatric cardiologists and cardiac surgeons, the spontaneous closure of these defects is very rare. The left ventricular-to-right atrial shunts cause these patients to have significant symptoms, and all of our patients had either congestive heart failure, failure to thrive, or exercise intolerance. The operation to close these defects is quite safe. The defect is away from the conduction system and in our series all patients were in normal sinus rhythm. There were no residual defects, no reoperations, and no significant tricuspid valve insufficiency. The Gerbode ventriculo-atrial defect is a rare defect with excellent surgical results.
References
- Buhl, cited by Meyer H. Uber angeborene Enge oder Verschluss der Lungenarterienbahn. Virchow’s Arch f path Anat 1857;12:532.
- Kirby CK, Johnson JJ, Zinsser HF. Successful closure of a left ventricular-right atrial shunt. Ann Surg 1957;145:392.
- Gerbode F, Hultgren H, Melrose D, Osborn J. Syndrome of left ventricular-right atrial shunt. Successful repair of defect in five cases, with observation of bradycardia on closure. Ann Surg 1958;148:433-46.
- Jacobs JP, Burke RP, Quintessenza JA, Mavroudis C. Congenital Heart Surgery Nomenclature and Database Project: ventricular septal defect. Ann Thorac Surg 2000;69(Suppl):S25-35.
- Riemenschneider TA, Moss AJ. Left ventricular-right atrial communication. Am J Cardiol 1967;19:710-8.
- McKay R, Battistessa SA, Wilkinson JL, Wright JP. A communication from the left ventricle to the right atrium: a defect in the central fibrous body. Int J Cardiol 1989;23:117-23.



