
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Dual Right Second Rib and Clavicle Fracture Fixations

Rib fractures have been reported to occur in 20 percent of patients with thoracic trauma (1). A second rib fracture indicates high-impact trauma and is usually associated with clavicle and scapular fractures.
A fracture of the second rib is associated with high probability of injury to the subclavian vessels, branches of the brachial plexus, and lung injury, either pneumothorax or hemothorax.
A combined clavicle and second rib fracture may lead to costo-clavicular instability complex, which may increase the chance of developing thoracic outlet syndrome and chronic pain syndrome.
Surgical Case
A 65-year-old woman known to have fibromyalgia was exposed to a high-velocity road traffic accident. She experienced severe chest pain, shortness of breath, and subcutaneous emphysema. After the primary survey, a chest computed tomography scan showed a right first non-displaced rib fracture posteriorly, displaced clavicle, and right second rib fractures with significant displacement (Figure 1), associated with pneumo-hemothorax and subcutaneous emphysema, along with upper lobe lung contusion.
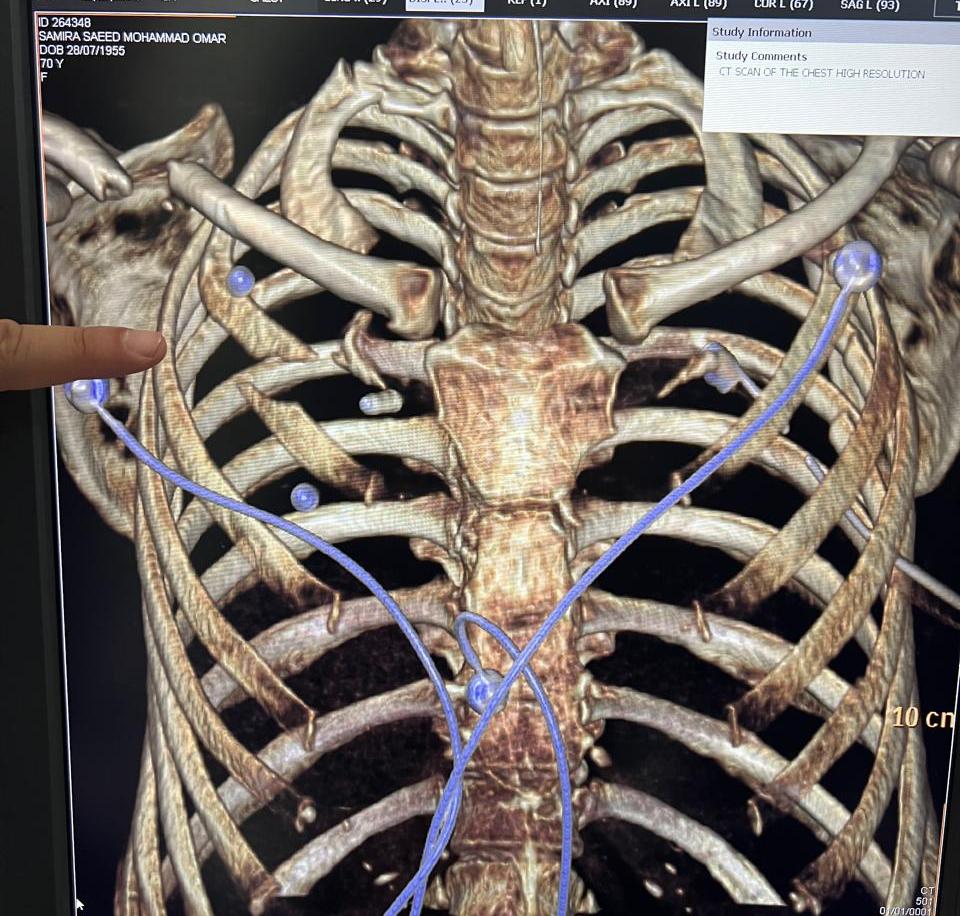
Figure 1: A chest 3D reconstruction scan, which delineates a significantly displaced anterior right second rib fracture and clavicle, as well as a non-displaced first rib fracture posteriorly.
Operation
While the patient was in a supine position, the surgeons kept the right arm and forearm in a mobile position to help with localization of the rib fracture and to assess dynamic stability of both the clavicle and rib fracture. An oblique incision of 5 cm, with a total length of 7 cm, was made using an infraclavicular approach parallel to the right clavicle (Figure 2).

Figure 2: Right infraclavicular approach with a 7 cm incision.
The procedure involved cutting the skin and subcutaneous tissue, splitting the pectoralis major muscle, and exposing the deltopectoral fascia. Dissection of the right axillary vein was performed, along with the ligation of the thoracoacromial and cephalic branches using 0 silk ties (Figure 3).

Figure 3: Dissection of the right axillary vein.
Vessel loops were applied around the dissected axillary vein for retraction of the vein. The sites of the second rib fracture, located below the axillary vein, were then identified (Figure 4).
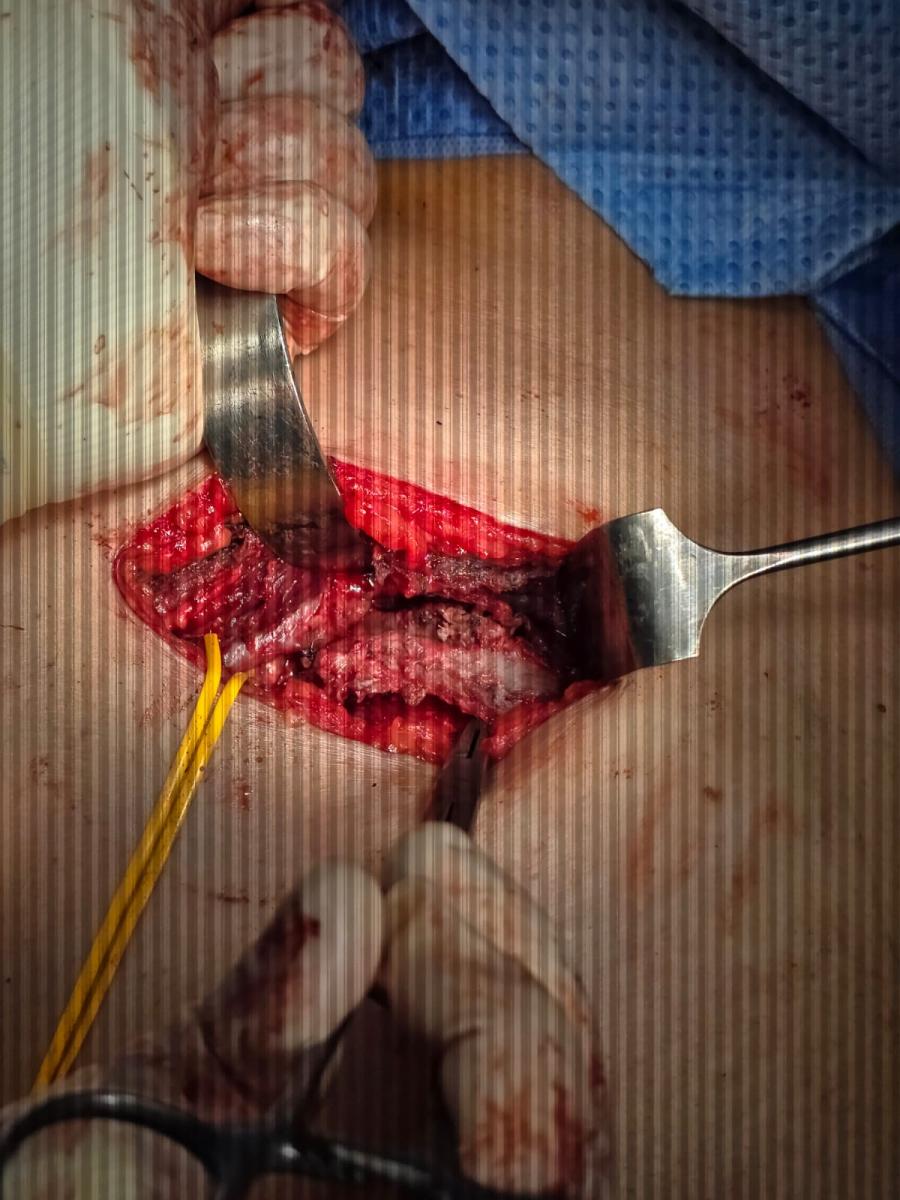
Figure 4: Identification of the proximal and distal sites of the second rib fractures.
Preserving the intercostal neurovascular bundle then occurred and a large titanium rib plate was used (Figure 5).
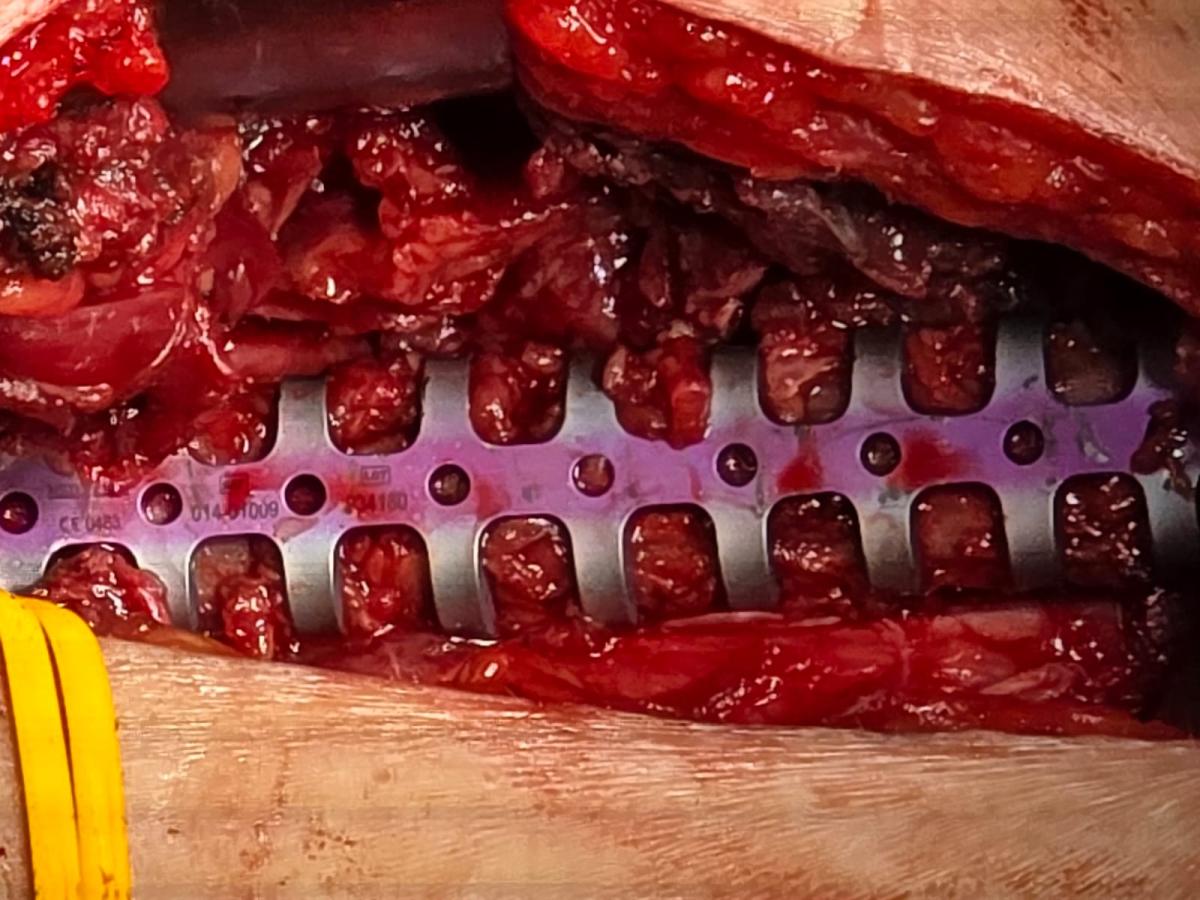
Figure 5: Fixation of the second rib fracture using a titanium plate.
The orthopedic surgeon used a subcutaneous approach via the same incision to fix the clavicle using an anatomical locking compression clavicle plate and screws (Figures 6A and 6B).

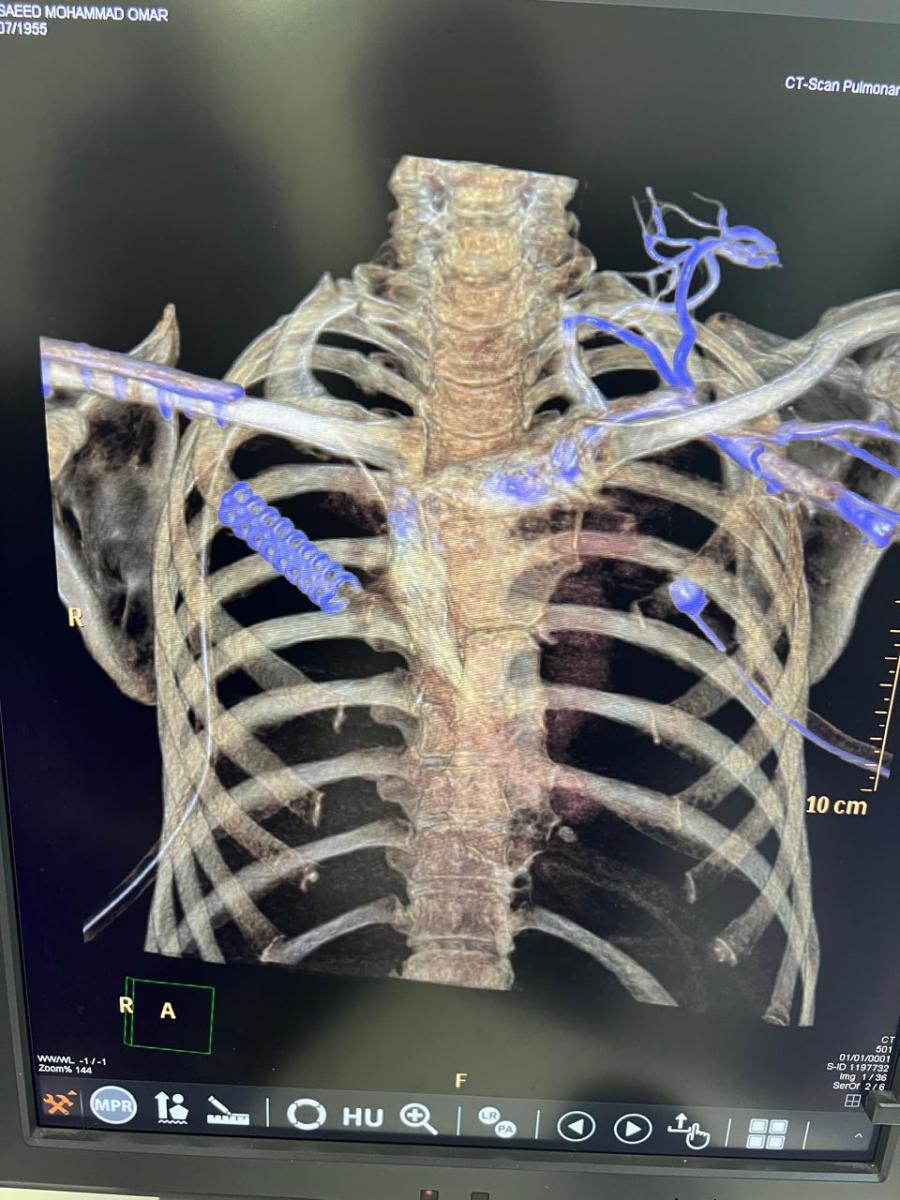
A B
Figures 6A and 6B: A- Lateral view of a 3D reconstructed CT scan after clavicle and second rib fixation; B- Anterior view of a 3D reconstructed CT scan after clavicle and second rib fixation.
Hemostasis was secured, and the wound was closed in layers. The patient was doing well after surgery and started physiotherapy without experiencing any pain.
Discussion
Early rib fracture fixation is superior to late stabilization in minimizing hospital stays and complications, as well as enabling a faster return to baseline health status.
Many hardware options can be used for rib fixation (1), including:
- Plating with cortical screws
- Absorbable plating
- Judet struts
- Kirschner wires
- Intramedullary rods
Tips and Pitfalls
- The periosteum of the rib should remain in place and not be excessively dissected to promote healing.
- A preoperative computed tomography scan with 3D reconstruction is recommended for surgical planning.
- Fixation of the second rib fracture is technically demanding due to the location of the second rib, which is deeper than the subclavian vessels and axillary vein and close to the brachial plexus.
- Preservation of the intercostal neurovascular bundle is essential to avoid chronic pain syndrome.
The most common ribs for plating are the fourth through 10th ribs because they are the most mobile and painful. However, the first two ribs are more difficult to access (2). There are some specific indications for rib plating of the second rib, such as (2):
- If the rib fracture is associated with significant displacement and a marked gap
- If there is an accompanying subclavian vascular injury or brachial plexus injury
- If there is an association with neurological deficit
- For flail chest with upper anterior chest wall instability, which can be radiological or clinical and adds paradoxical movement of the chest cage during respiration
- Malunion or nonunion with chronic pain syndrome
- Mechanical clicking
Conclusion
Dual fixation of the second rib and clavicle fracture is technically demanding but stabilizes the costo-clavicular complex, which minimizes the incidence of thoracic outlet syndrome and chronic pain syndrome.
References
- Rib fixation: Who, What, When? Marc de Moya et al. Trauma Surg Acute care 2017 Apr;2: e000059.
- Surgical stabilization of rib fracture (SSRF): the WSES and CWIS position paper. G sermonesi et al. World J Emerg Surg. 2024.
Disclaimer
The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.



