
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Management of Chronic Neglected Traumatic Diaphragmatic Hernia
Ahmed MSM, Abdelaal K, Abdelgaffar A, et al.. Management of Chronic Neglected Traumatic Diaphragmatic Hernia. February 2019. doi:10.25373/ctsnet.7662950.

Figure 1. Chest x-ray, suggestive of tension pneumothorax.
A 45-year-old man came to the emergency department complaining of progressive shortness of breath for 10 days. He also complained of vomiting and absolute constipation for four days. He had a past history of left stab to the chest for 1.5 years. Examination revealed the patient was hemodynamically unstable, with severe respiratory distress, cyanosis, fever, and absent air entry on the left side of the chest. The patient had a chest x-ray suggestive of tension pneumothorax, however a chest computed tomography scan was suggestive of diaphragmatic hernia.
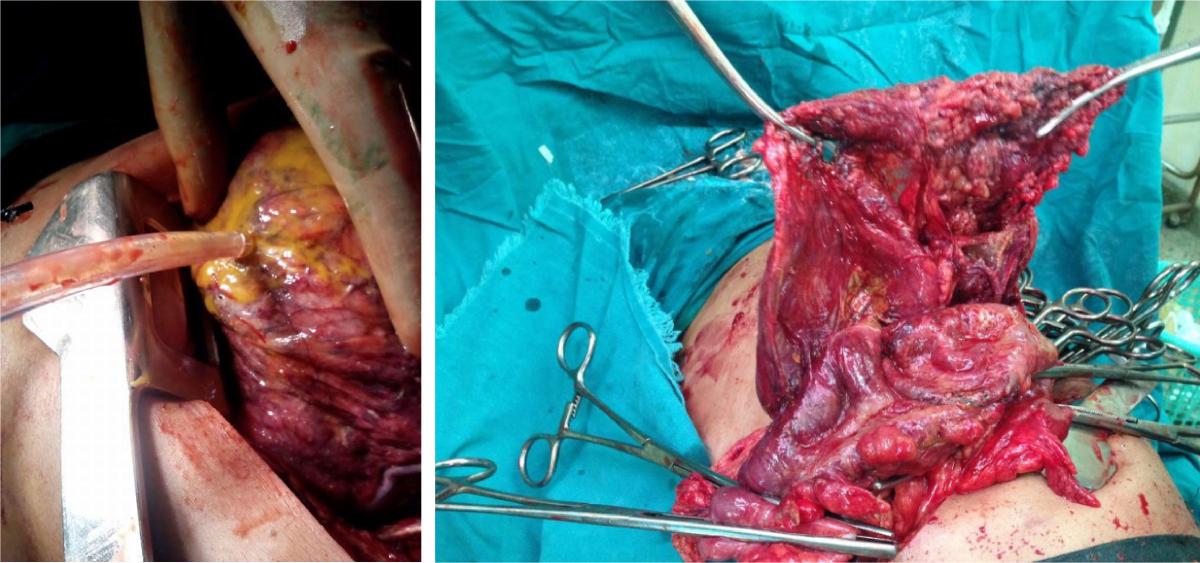
Figure 2. Left posterolateral thoracotomy revealed a gangrenous perforated transverse colon.
An emergency left posterolateral thoracotomy was performed. There was a gangrenous perforated transverse colon inside the chest. The authors widened the diaphragmatic defect, and they performed a transthoracic transverse colectomy and reanastomosis, as well as a right iliac ileostomy. The authors repaired the diaphragmatic defect. The patient was discharged at postoperative day 30 in a good general condition.

Figure 4. The chest was closed in the usual manner.
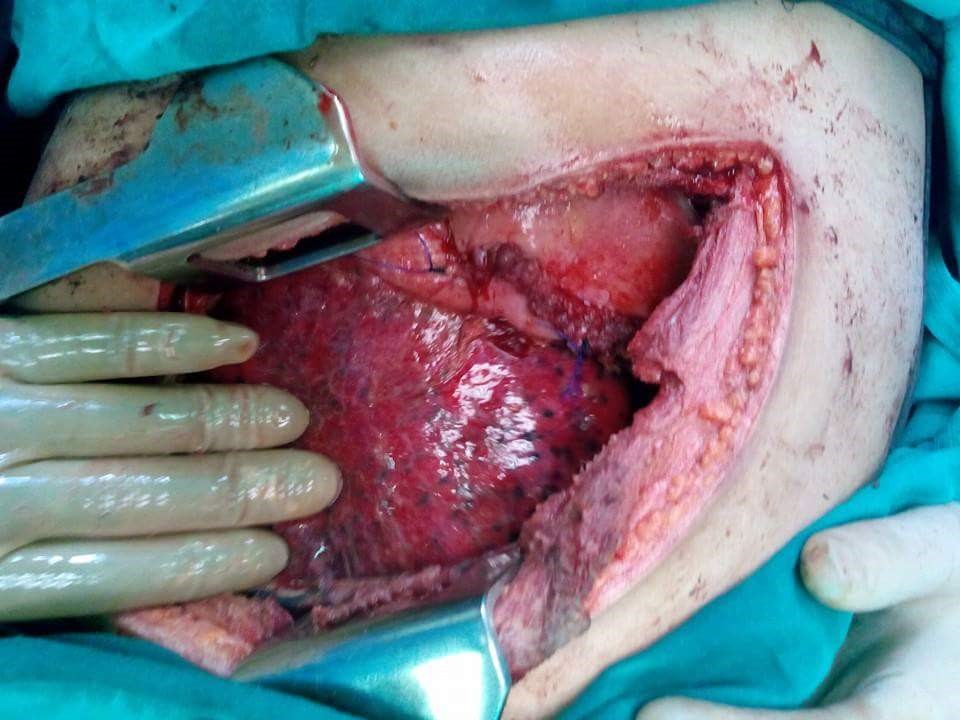
Figure 3. The diaphragmatic tear was closed in two layers with polypropylene suture.
Conclusion
History-taking and high index of suspicion is important for the diagnosis of neglected traumatic diaphragmatic injuries. In this case, the authors performed the repair totally transthoracically, with no need for an abdominal incision.



