
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Nail Gun Impacted in the Chest Wall: Report of a Failed Trail of Home Extraction by Patient’s Relatives
Mohamed EE, El-Ghaffar AMA, Aal KMA, Afifi TM, Abdelaziz AA, Ahmed MSM. Nail Gun Impacted in the Chest Wall: Report of a Failed Trail of Home Extraction by Patient’s Relatives. April 2019. doi:10.25373/ctsnet.8009438.
Introduction
A pneumatic nail gun is an alternative tool to a hammer. This useful device has been used since 1959 to fire nails into wood and other surfaces at high speed [1, 2]. In spite of its convenience, life-threatening and fatal nail gun injuries can occur when the operator has insufficient training. Injuries by nail guns are rarely reported, but an increase in the rate of use of nail guns is directly related to an increase in nail gun injuries [3]. Nail gun injuries to the neck and chest are rare accidents but are important and increasing in frequency [4]. Nail gun injuries, mostly reported in adult men, are most commonly due to work-related accidents [5], but self-inflicted injuries are also reported [2]. Aliyu and his colleagues reported a nail gun penetrating cardiac injury in a 4-year-old Nigerian girl [6]. The authors report their experience in the management of a man who was injured by an accidental shooting of a nail gun while working in roof construction. In that accident, a nail penetrated the patient’s sternum. This case provides interesting and rare imaging findings, demonstrating a nail penetrating the sternum in a vertical way, with no cardiovascular compromise.
Case Presentation
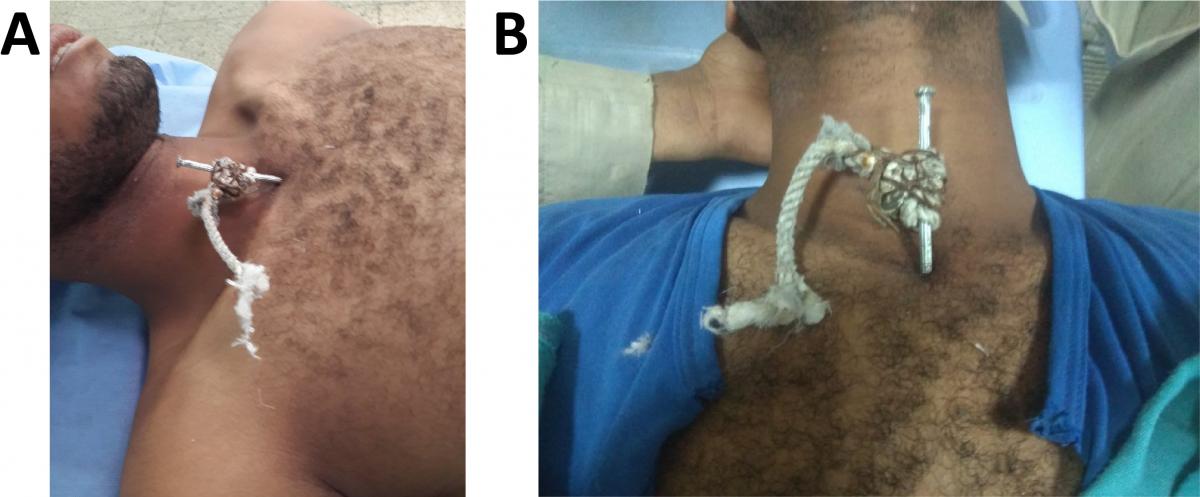
Figure 1. A) A 10 cm stainless steel pin impacted at the manubrium, caused by a nail gun accident during construction work. B) A 10 cm stainless steel pin impacted at the manubrium.

Figure 2. Computed tomography of the chest, sagittal view showing the fired nail traversing the manubrium obliquely with the long axis of the nail parallel to the long axis of the neck. Just the nail tip in the superior mediastinum.
The visible part of the nail was about 6.5 cm in length. The patient was apprehensive, in great fear, and complained of severe pain. He was hemodynamically stable: blood pressure 142/85, pulse rate 122 in sinus rhythm, SO2 98 % on room air, and slightly tachypneic. Physical examination demonstrated heart sounds that were audible with no abnormalities detected except tachycardia, good air entry bilaterally on auscultation, neck veins that were not engorged, and no bleeding from the site of nail impaction. The authors noticed a rope was tied by multiple knots to the exposed part of the nail. When asked about that, the patient said his peers tried to extract the nail with the aid of this rope, but they failed. In the emergency department the authors inserted intravenous (IV) cannulae, performed routine laboratory investigations, and obtained blood grouping and matching. The patient received antibiotics, analgesia, and antitetanus serum.

Figure 3. Nail directly extracted. Pressure at the penetration site to control bone bleeding.
Computed tomography (CT) of the chest with IV contrast revealed a nail penetrating the manubrium (Figure 2). The penetration was in a vertical orientation with slight oblique direction, with the entry point located at the superior end of the anterior plate (about 0.5 cm right of the sternal notch) and penetrating the mid part of the posterior plate as seen in the sagittal view of the CT scan, with just a few millimeters of the nail penetrating into the superior mediastinum. In the sagittal view of the CT scan, one can see fissure fracture of the posterior and anterior plates of the manubrium sterni at separate levels (Figure 2), so the stability of the sternum was not affected.
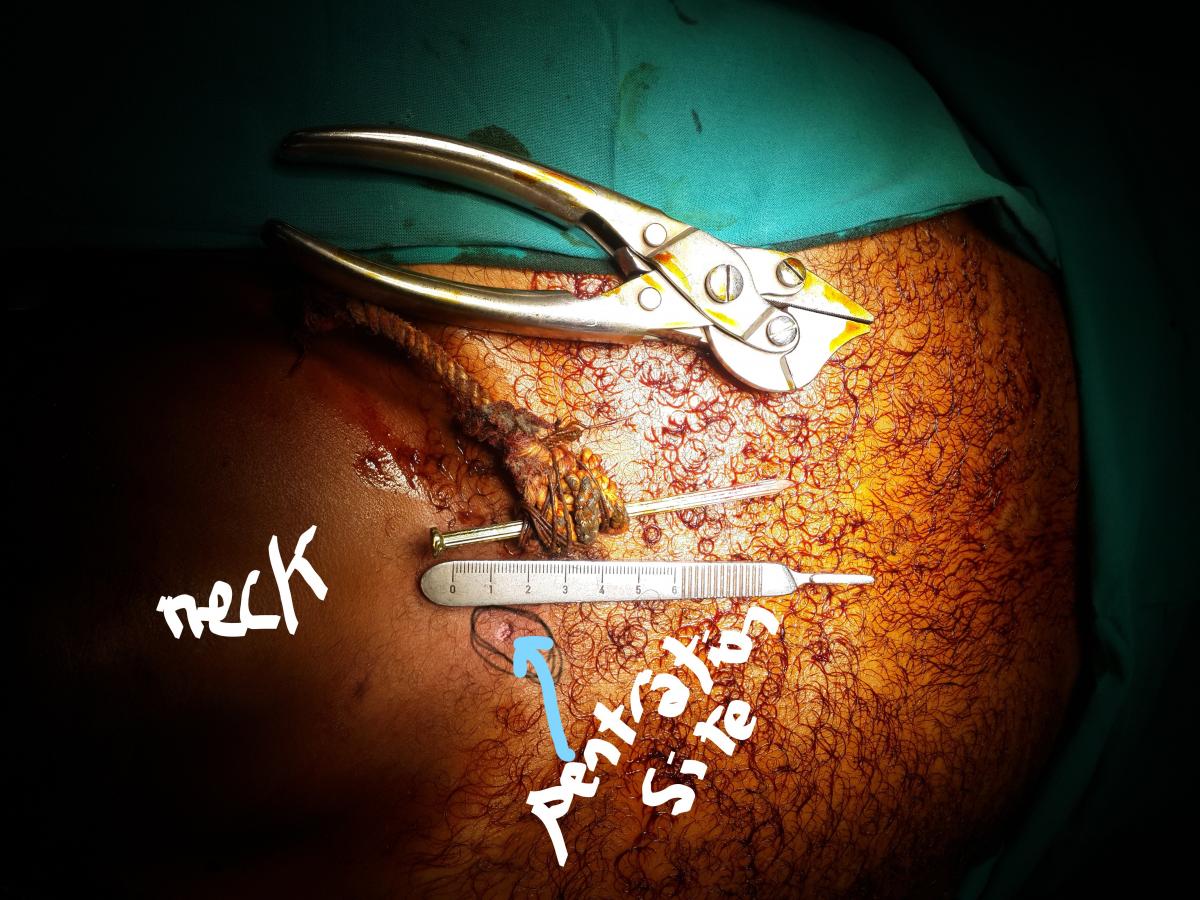
Figure 4. Illustration of the penetration site. The size of the nail is 10 cm. No bleeding from the penetration site.
The authors brought the patient to the operation room, as all physical findings and CT findings ruled out the presence of any cardiovascular or tracheal injury as the few millimeters penetration into the superior mediastinum was not enough to result in an internal injury. In the operation room, with the patient under general anesthesia without endotracheal intubation, the authors extracted the nail without exploration (Figure 3), although they were ready to explore if the indication arose. The extraction went smoothly and was uneventful with no bleeding (Figure 4). The total length of the nail was 10 cm. A follow-up CT was performed, and the patient was kept under observation for 24 hours and then discharged home.
Discussion
Most nail gun injuries are due to work accidents, but sometimes they are self-inflicted as a suicide attempt [2]. Chest CT scans can be used to confirm the intrathoracic position of the nail and to detect a pericardial effusion [7]. The presence of pericardial tamponade indicates the need for emergent surgical intervention via median sternotomy or thoracotomy according to the location of cardiac injury [8]. Nail gun penetrating chest and neck injuries are rare entities in the literature, and this mechanism of injury is mostly work related [9]. The management of nail gun injuries to the chest and neck is challenging because the effect of the injury is highly variable, ranging from just extraction of the nail as in this situation and other reports [4, 9] to a life threatening situations like cardiac tamponade and other cardiac injuries [2, 6, 10, 11].
This patient was fortunate, as the nail penetrated the sternum for about 3.5 cm in a vertical direction and only the tip of the nail was in the superior mediastinum, away from vital structures. The chest CT saved the patient from unnecessary exploration. In such rare situations, nail gun injury to the chest happens with no significant sequelae.
In the authors’ opinion, the variability of the effect of the injury is related to many factors: the length and thickness of the nail, the direction of penetration, the power of the firing gun and its distance from the victim, time lag from the accident to hospital presentation, hospital facilities, and the wise management of the patient from the time of accident until hospital arrival. In this situation (Figure 1), we noticed a rope fixed around the nail that was related to a failed attempt by the patient’s relatives to extract the nail by pulling on the rope at the scene of the accident. In fact, the relative’s trial is very risky and should not be done.
Nail guns have been in use since 1959 in Western countries [2]. In Egypt, their use is increasing in recent years. We expect an increasing number of this type of accident in our locality. This is the first case of nail gun injury to the neck and chest presenting at our hospital. To our knowledge, it is the first case to be reported in the literature in which the nail penetrating in this location in the chest, just below the root of the neck and in a vertical manner, parallel to the long axis of the neck. This direction may have been the most important determinant of the nonfatal outcome in this case. It also is the first report in which extraction was attempted at the scene of accident by tying a rope around the nail and applying traction on the rope.
Conclusion
Nail gun is a rare but important cause of penetrating chest trauma. Cardiac nail gun injury is a life threatening injury. If the patient is unstable, immediate intervention (thoracotomy or sternotomy) helps reduce the rate of mortality. In stable patients, a high index of clinical suspicion and use of the best and fastest imaging modalities are helpful for successful management. Adequate training and application of safety measures are essential to prevent accidental nail gun injuries.
References
- Beaver AC, Cheatham ML. Life-threatening nail gun injuries. Am Surg. 1999;65(12):1113-1116.
- Ho S, Liu B, Feranec N. Self-inflicted cardiac injury with nail gun without hemodynamic compromise: a case report. Cureus. 2017;9(1):e971.
- Tuladhar S, Eltayeb A, Lakshmanan S, Yiu P. Delayed presentation of right and left ventricle perforation due to suicidal nail gun injury. Ann Card Anaesth. 2009;12(2):136-139.
- Jong Soon H, et al. A case study of a patient with penetrating neck injuries caused by a nail gun. J Korean Soc Traumatol. 2011;24(1):48-51.
- Willem Guillermo Calderon M, et al. Penetrating cardiac injury and traumatic pericardial effusion caused by a nail gun. J Korean Soc Traumatol. 2017;30(1):21-23.
- Aliyu I, Inuwa I. Nail in the heart of a 4-year-old Nigerian girl. Nigerian J Cardiol. 2013;10(2):85-87.
- Jodati A, Safaei N, Toufan M, Kazemi B. A unique nail gun injury to the heart with a delayed presentation. Interact Cardiovasc Thorac Surg. 2011;13(3):363-365.
- Eren E, Keles C, Sareyyupoglu B, Bozbuga N, Balkanay M, Yakut C. Penetrating injury of the heart by a nail gun. J Thorac Cardiovasc Surg. 2004;127(2):598.
- Bigder M, Zeiler F, Berrington N. Nail-gun injury through the spinal canal. Can J Neurol Sci. 2015; 42(3):203-204.
- Mubark YS, Farghaly AM. Accidental nail gun penetration to right ventricle: a case report. J Cardiol Cardiovasc Ther. 2017;3(4):555618.
- Takagi H, Mori Y, Murase K, Hirose H. Nail gun penetrating cardiac injury. Eur J Cardiothorac Surg. 2003;23(5):841.



