
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Peroral Endoscopic Myotomy (POEM)
While the standard of care for patients with achalasia remains laparoscopic modified Heller myotomy with partial fundoplication, there are many options available for patients to consider. Neither balloon dilatation nor injection of Botox provides as sustainable relief, and both often require repeat intervention. In addition to providing only short-term results, these options cause scar tissue to develop that may complicate a laparoscopic repair by increasing the perforation rate and making a complete myotomy difficult.
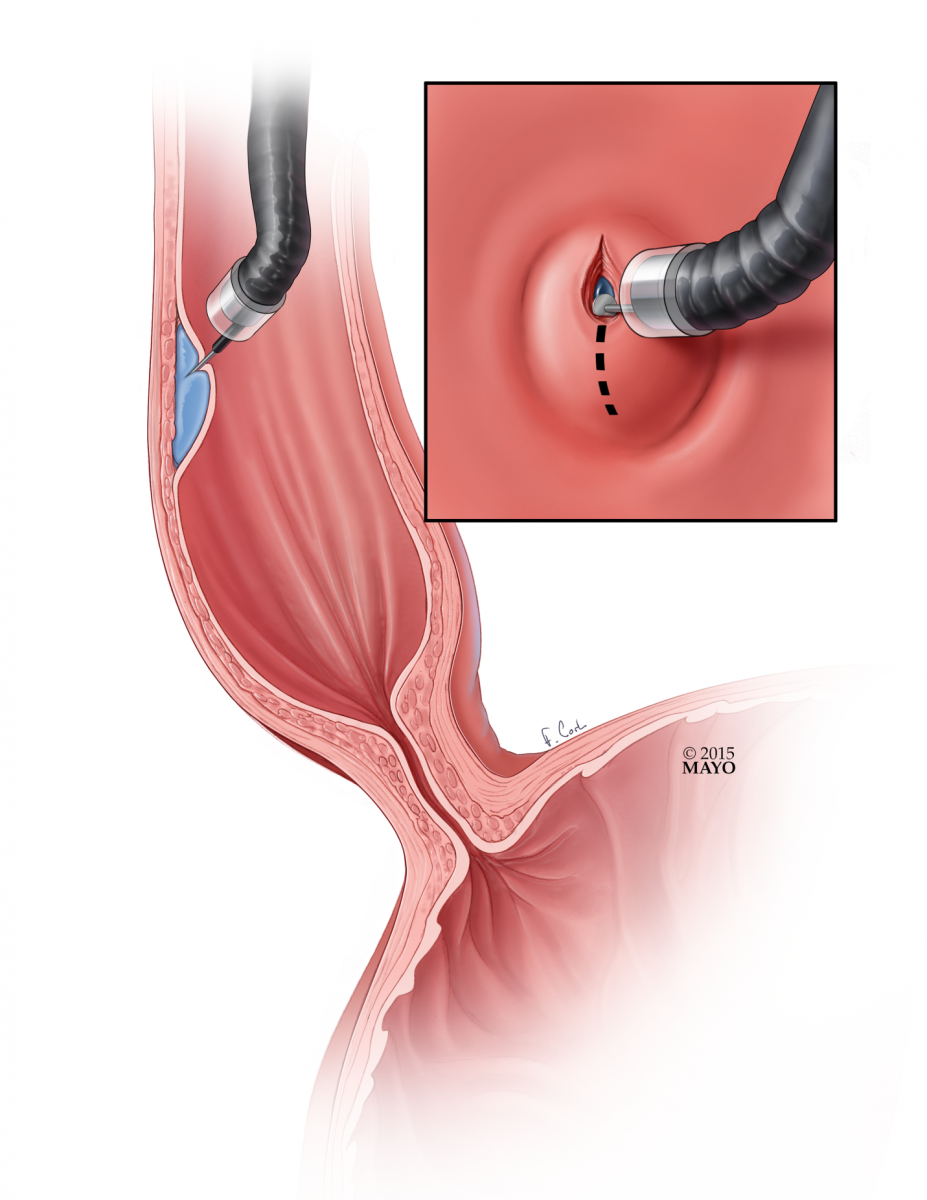
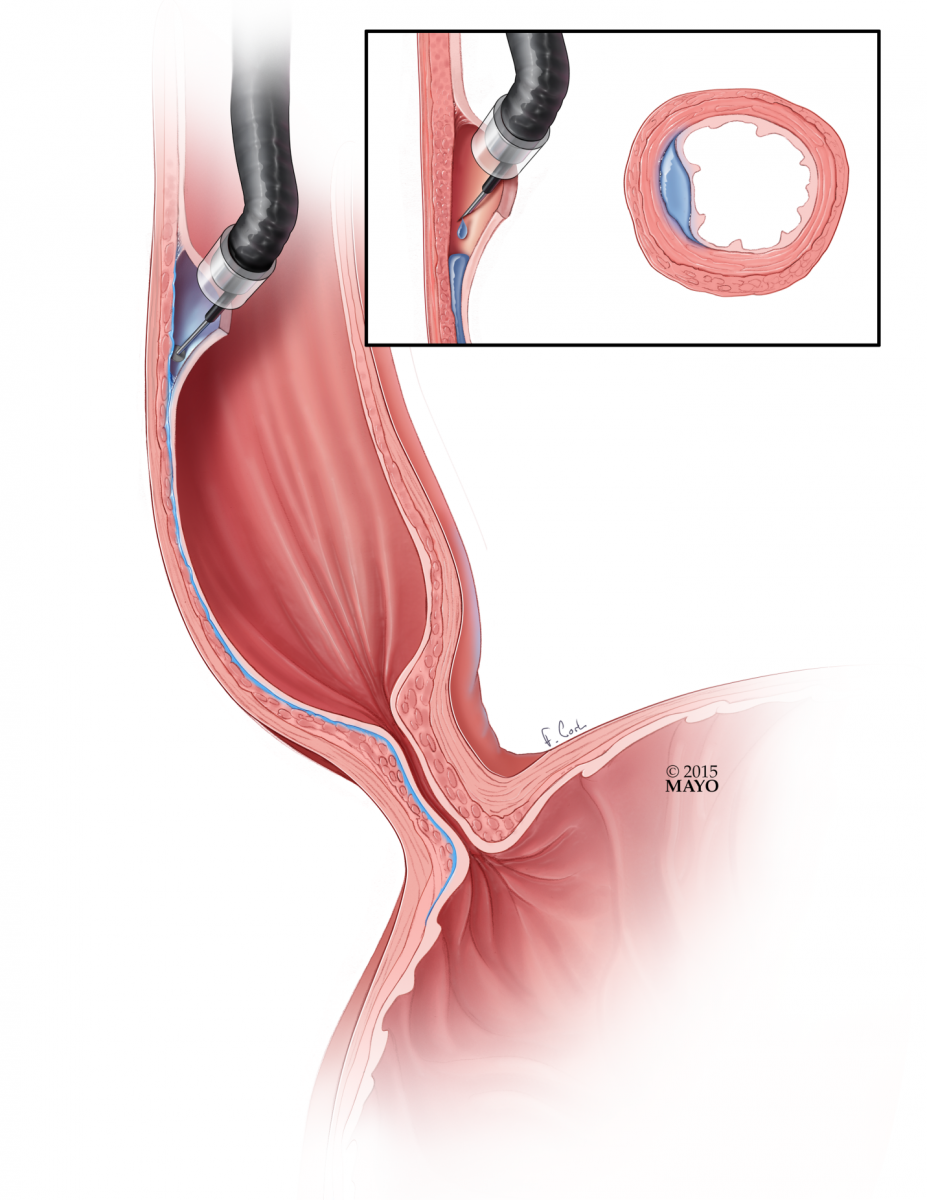
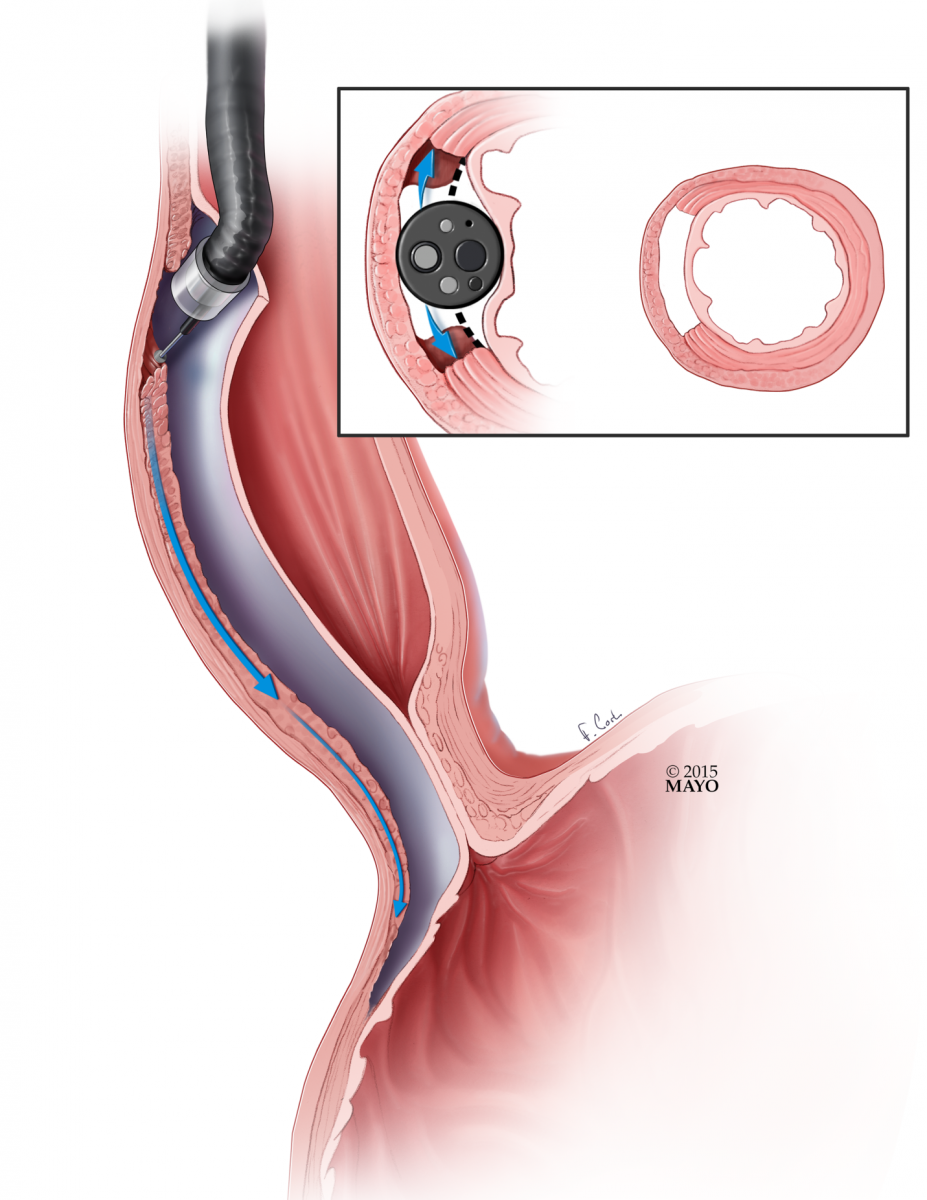
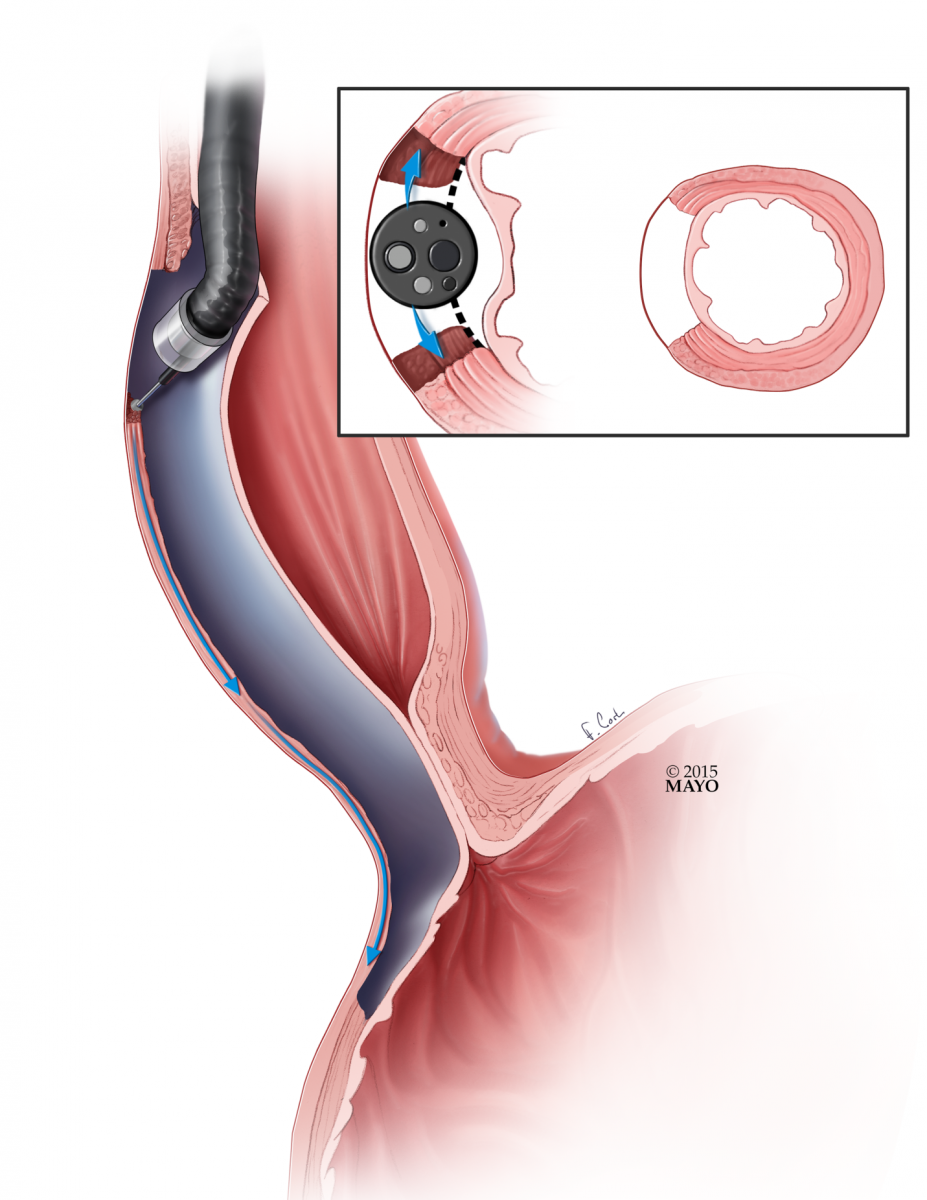
A newer option, available in specialized centers, is peroral endoscopic myotomy (POEM). POEM is a totally endoscopic procedure, utilizing the advanced endoscopic technique of submucosal tunneling. Once positioned well above the UES (upper esophageal sphincter), a submucosal fluid cushion is created and an incision is made with an endoscopic knife (Figure 1). The scope is advanced into the submucosal layer of the esophagus (Figure 2). Using water jet injection, suction, low-dose energy ablation, and blunt dissection, the scope is advanced past the esophago-gastric junction in the submucosal plane (Figure 3). Either a myotomy limited to the circular muscle (Figure 4) or a full thickness myotomy (Figure 5) is then performed. The mucosal incision is then closed with hemostatic clips (Figure 6).
Advantages of the endoscopic myotomy include a potentially longer myotomy than one would be able to create with a laparoscopic approach alone, and a completely endoscopic approach in the setting of no follow-up laparoscopy. The potential disadvantages of POEM include no long-term data to understand the natural course after POEM, and the unresolved issue of reflux post-POEM. Further controversies include where to perform the myotomy, and methods to confirm adequate extension onto the stomach. Further data needs to be acquired in order to consider POEM equivalent to the laparoscopic myotomy.
 |
 |
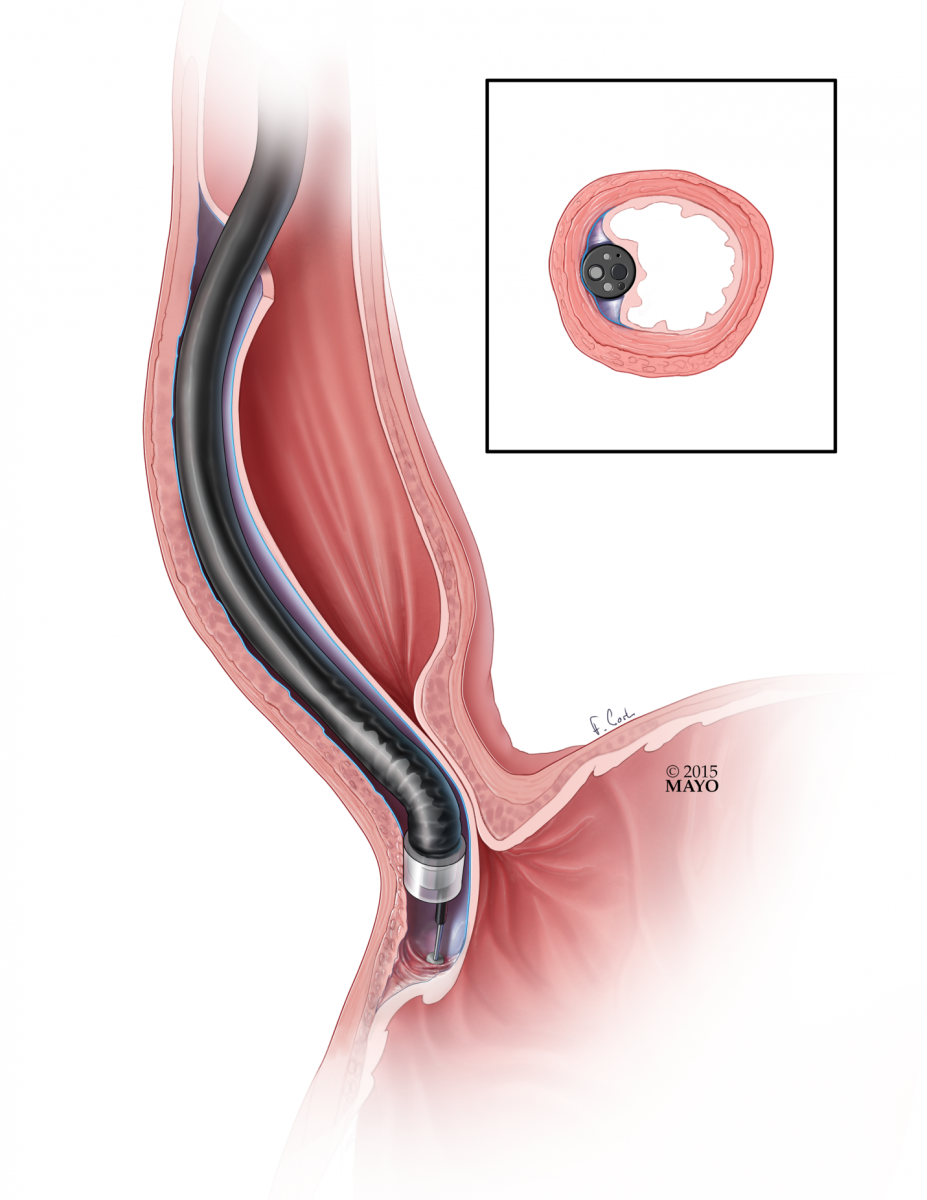 |
| Figure 1: Submucosal injection to create submucosal fluid cushion. | Figure 2: Creation of submucosal working space. | Figure 3: Submucosal tunnel. |
 |
 |
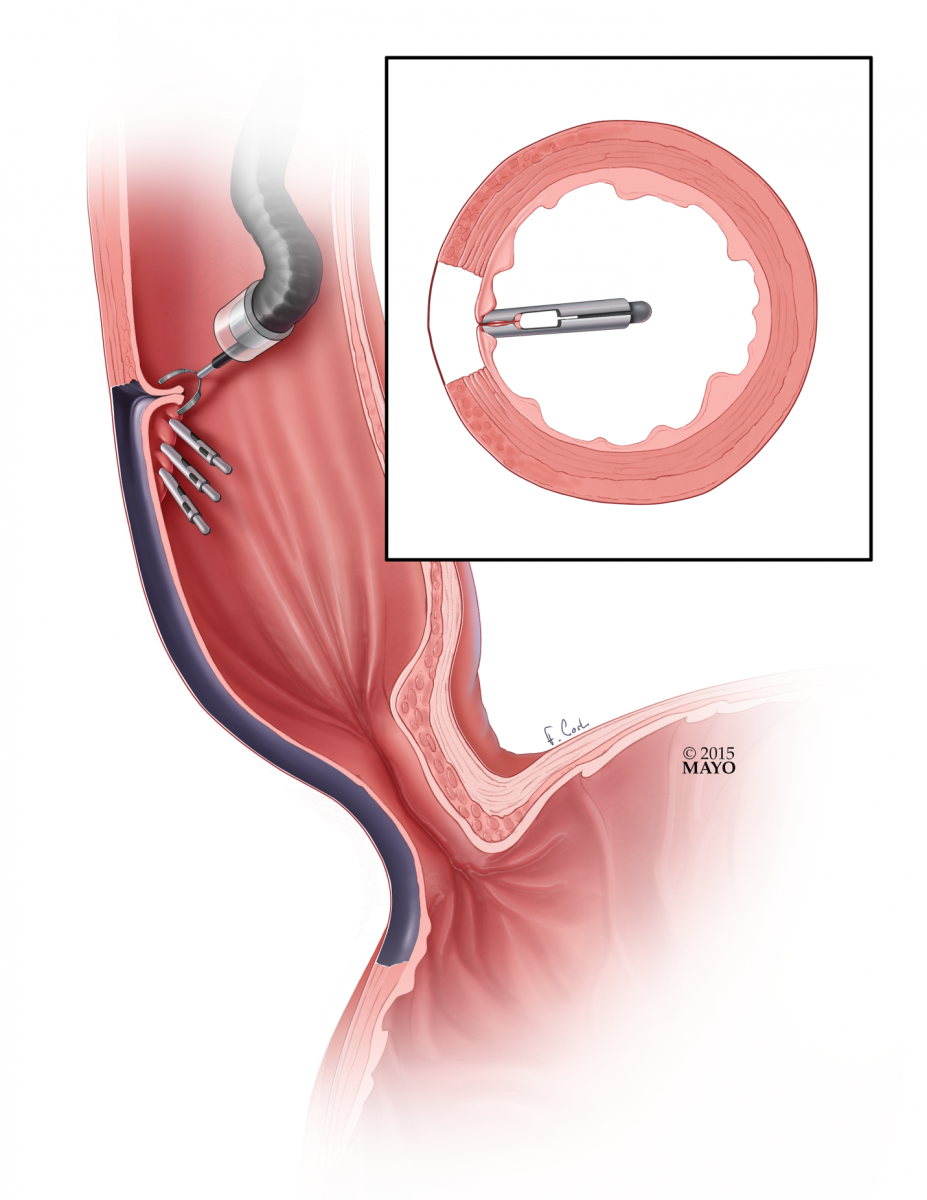 |
| Figure 4: Circular muscle myotomy. | Figure 5: Longitudinal muscle myotomy. | Figure 6: Closure of mucosal incision. |
Suggested reading:
- Stavropoulos SN, Desilets DJ, Fuchs KH, Gostout CJ, Haber G, et al. Per-oral endoscopic myotomy white paper summary. Gastrointestinal Endoscopy. 2014; 80(1):1-15
- Stavropoulus SN, Modayil RJ, Friedel D, Savides T. The International Per Oral Endoscopic Myotomy Survey (IPOEMS): a snapshot of the global POEM experience. Surg Endosc 2013; 27:3322-3338
- Swanstrom LL, Kurian A, Dunst CM, Sharata A, Bhayani N, Rieder E. Long-term outcomes of an endoscopic myotomy for achalasia: the POEM procedure. Ann Surg. 2012 Oct;256(4):659-67.
- Verlaan T, Rohof WO, Bredenoord AJ, Eberl S, Rösch T, Fockens P. Effect of peroral endoscopic myotomy on esophagogastric junction physiology in patients with achalasia. Gastrointest Endosc. 2013 Jul;78(1):39-44.
- Inoue H, Minami H, Kobayashi Y, Sato Y, Kaga M, Suzuki M, Satodate H, Odaka N, Itoh H, Kudo S. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010 Apr;42(4):265-71.




Comments