
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Mitral Valve Replacement on a Beating Heart in a Patient With a Porcelain Aorta
Porcelain aorta, characterized by extensive circumferential or near circumferential calcification of the ascending aorta, poses a significant risk for embolic events during conventional cardiac surgery requiring aortic cannulation, cross-clamping, and cardioplegia (1). Surgical options include off-pump techniques, alternative perfusion strategies, and transcatheter approaches (2). Beating heart surgery is another alternative with favorable morbidity and mortality results in otherwise inoperable cases (3). The authors report a case of mitral valve replacement on a beating heart to circumvent the complications associated with porcelain aorta.
Case Presentation
A 40-years-old female presented with progressive dyspnea (NYHA III), orthopnea, and lower limb edema. An echocardiography revealed severe mitral regurgitation (MR), moderate to severe tricuspid regurgitation (TR), an ejection fraction (EF) of 70 percent, and a pulmonary artery systolic pressure (PASP) of 55 mmHg.
She had a history of hypertension and cachexia. The chest X-ray raised suspicion of aortic calcification, confirmed by a noncontrast CT scan, which demonstrated severe circumferential aortic calcification (porcelain aorta) with calcification-free femoral arteries (figures 1, 2).
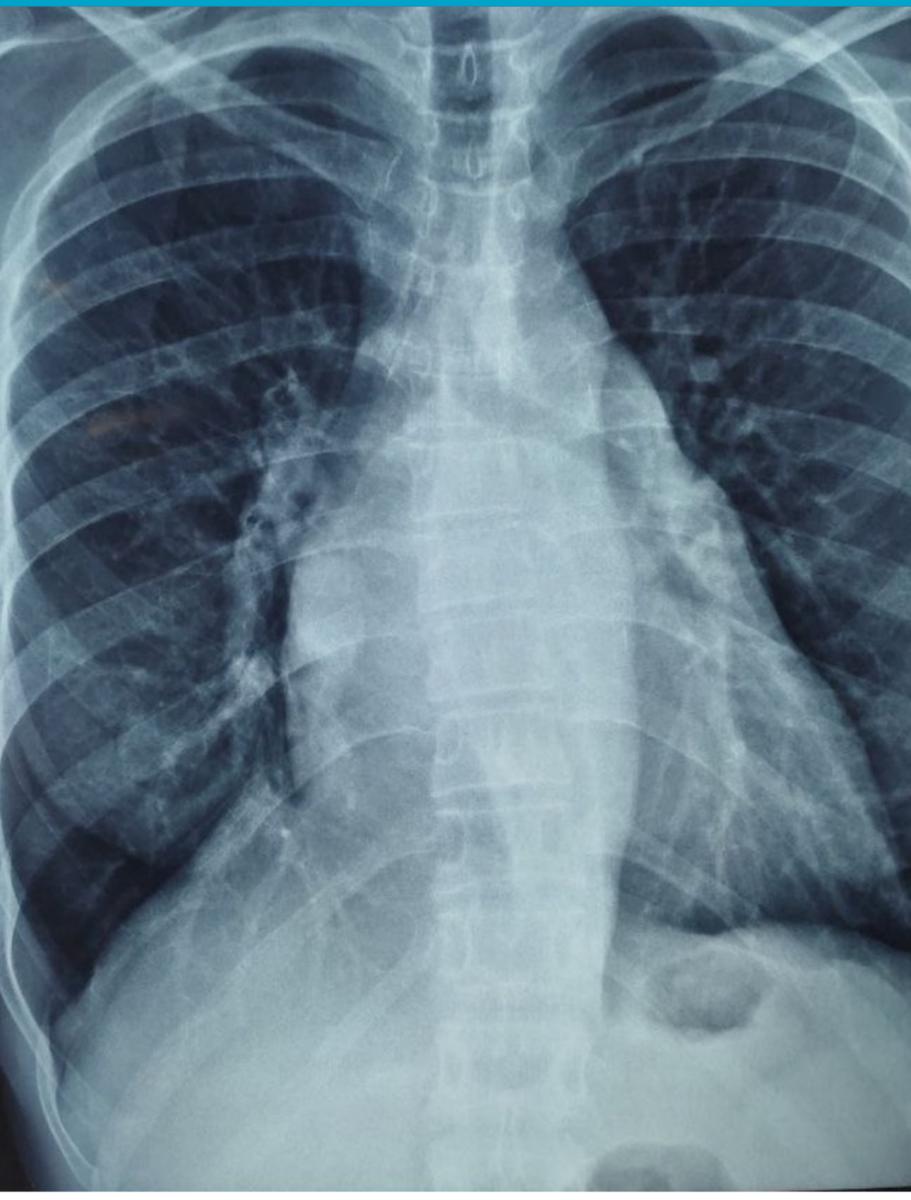
Figure 1: CXR showing the porcelain aorta.

Figure 2: CT showing the porcelain aorta.
Surgical Technique
The approach involved a median sternotomy, along with right femoral arterial and bicaval venous cannulation. The beating-heart strategy included no aortic cross-clamping and cooling the patient to 28-degress Celsius to induce bradycardia. An intracardiac bullet vent was placed through the left atrium into the left ventricle to minimize the risk of air embolism.
Valve Replacement and Repair
The mitral valve was replaced with a 25 mm mechanical prosthesis, while preserving the basal chordae of the posterior leaflet. Additionally, the tricuspid valve was repaired using the De Vega technique.
Postoperative Course
The patient was weaned off bypass easily on Milrinone and a low dose of Noradrenaline, maintaining sinus rhythm. Recovery was uneventful, and she was discharged on postoperative day five in stable condition.
At the follow-up, the patient demonstrated marked clinical improvement with resolution of dyspnea and lower limb edema.
Discussion
Porcelain aorta remains a high-risk factor in cardiac surgery, with aortic manipulation increasing the risk of stroke and embolism (4). In this case, avoiding aortic cross-clamping was critical to preventing complications.
Key Surgical Considerations for Porcelain Aorta
1. Avoiding Aortic Manipulation
Traditional MVR involves cannulating and cross-clamping the aorta and cardioplegic arrest, which increases the risk of embolization and stroke in patients with porcelain aorta.
Beating-heart surgery with femoral arterial cannulation provides a safer alternative.
2. Myocardial Protection Without Cardioplegia
Inducing bradycardia by cooling the patient to 28-degrees Celsius allowed for controlled beating-heart conditions (5). Maintaining coronary perfusion ensured adequate myocardial oxygenation.
3. Alternative Approaches
Some studies recommend transcatheter mitral valve replacement (TMVR) or minimally invasive MVR for these patients; however, these options may not be feasible in low-resource settings (6). This case reinforces the safety and feasibility of performing MVR on a beating heart in patients with porcelain aorta.
Conclusion
Beating-heart MVR is a viable surgical alternative for patients with porcelain aorta, as it reduces the risk of embolization while maintaining myocardial protection. Further studies are needed to establish the long-term outcomes of this approach.
Disclaimer
The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.




Comments