
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Emergency Lobectomy for Congenital Lobar Emphysema
Jan A, Tariq M, Shah SM, Khan AM, Anwar K, Khan A. Emergency Lobectomy for Congenital Lobar Emphysema. April 2019. doi:10.25373/ctsnet.7979714.
Introduction
Congenital lobar emphysema (CLE), also called congenital alveolar overdistension, is a birth defect of the lower respiratory tract. CLE causes hyperinflation of the pulmonary lobes. It can involve one or multiple lobes (1). It is a rare disease with a prevalence of 1 in 20,000 to 1 in 30,000 (3). Patients are diagnosed with this problem mostly as newborns or young infants, but less frequently the disease may be latent until adulthood. Approximately 25% of patients present at birth, 50% by one month of age, and the rest by six months of age. Common symptoms include tachypnea and increased work of breathing, and this can progress to cyanosis (2). Some cases of congenital lobar emphysema may be caused by autosomal dominant inheritance, while others occur for no apparent reason (sporadic).
Case Report
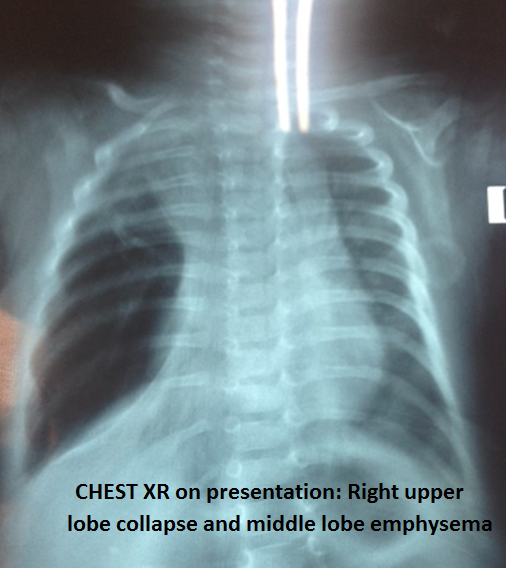
Figure 1. Chest x-ray demonstrating right upper lobe collapse and middle lobe emphysema.
A 1-month-old patient presented to the emergency room with difficulty breathing. On further history and examination, it was found that patient had a normal birth. The patient was up to date on vaccination and being breastfed. For last few days, the patient was having some difficulty feeding. On the day of admission, the patient was looking distressed to the parents. On examination, the patient was having labored breathing and was having decreased breath sounds in the left chest. The patient had a chest x-ray done with immediate impression for a possible right tension pneumothorax (Figure 1).
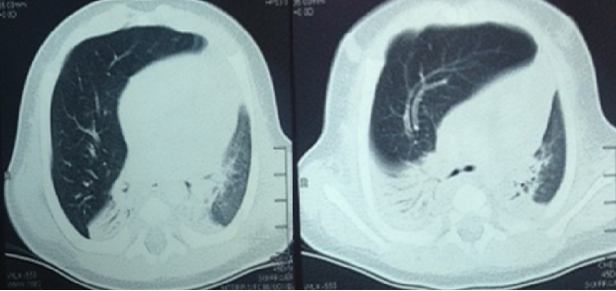
Figure 2. CT scan of the chest showing right middle lobe emphysema, collapse of the right lower and upper lobes, and mediastinal shift to the left side.
Urgent thoracic evaluation was acquired. The thoracic surgery team determined the presence of lung vascular markings in the right side, raising suspicion of congenital lobar emphysema. The patient rapidly progressed to respiratory distress requiring initiation of mechanical ventilation, hence an urgent computed tomography (CT) scan of the chest was performed. This confirmed the diagnosis of congenital lobar emphysema of the right middle lobe and mediastinal shift to the left (Figure 2).
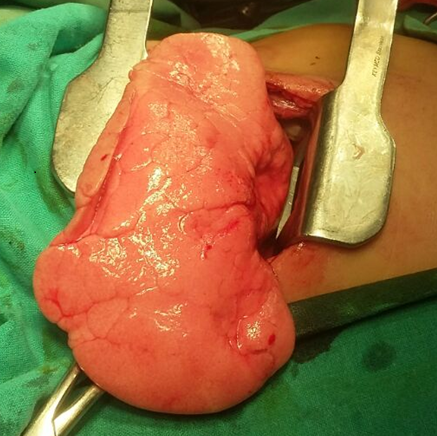
Figure 3. Intraoperative image of the very distended right middle lobe lying outside of the chest wall after incision.
The patient was transferred to the operating room and an emergent right middle lobectomy was performed through a posterolateral thoracotomy. Upon entering the thoracic cavity, it was obvious that the middle lobe was compressing the rest of the lung and the mediastinum. The distention was so much (as the patient was now on positive pressure ventilation) that the lobe spontaneously popped out of the incision (Figures 3 and 4).
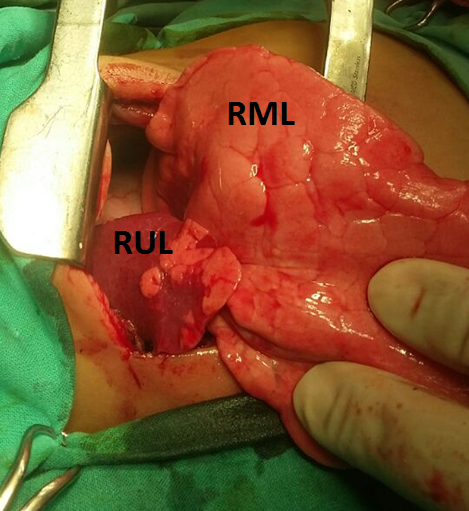
Figure 4. Intraoperative image of the right upper lobe.
The base of the lobe was clamped, and a few Valsalva maneuvers were given to re-expand the rest of the lung. Once the upper and lower lobes were expanded, a formal middle lobe lobectomy was performed. The patient was extubated on the first postoperative day and chest tubes were removed after confirmation of the absence of air-leak and complete lung expansion. The patient was discharged after an uneventful postoperative course and was completely stable on outpatient follow-up.
Discussion
Congenital lobar emphysema may be treated by observation alone in asymptomatic patients. If symptoms are present, then resection of the diseased lung can be done. It is a rare birth defect but chest x-ray can easily identify that the lung inflation is not normal. The differential diagnosis may include other lesions that are categorized as space-occupying, eg, congenital pulmonary airway malformation, bronchopulmonary sequestration, bronchogenic cyst, congenital diaphragmatic hernia, and Swyer-James-McLeod syndrome (unilateral hyperlucent lung syndrome) (2). A CT scan can be done quickly. It not only helps diagnose but also defines the anatomy and similarly rules out other differentials.
References
- Emphysema, Congenital Lobar. National Organization for Rare Disorders. URL https://rarediseases.org/rare-diseases/emphysema-congenital-lobar. Published 2003. Accessed April 9, 2019.
- Oermann CM. Congenital lobar emphysema. In: Hoppin AG, Garcia-Prats JA, Redding G. UpToDate. Alphen aan den Rijn, The Netherlands: Wolters Kluwer; 2019. URL: https://www.uptodate.com/contents/congenital-lobar-emphysema. Accessed April 9, 2019.
- Thakral CL, Maji DC, Sajwani MJ. Congenital lobar emphysema: experience with 21 cases. Pediatr Surg Int. 2001;17(2-3):88-91.



