
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Lung Infarct Following Lobectomy Mistaken for Gossypiboma: An Unusual Occurrence
Shenoy R. Lung Infarct Following Lobectomy Mistaken for Gossypiboma: An Unusual Occurrence. May 2019. doi:10.25373/ctsnet.8160230.
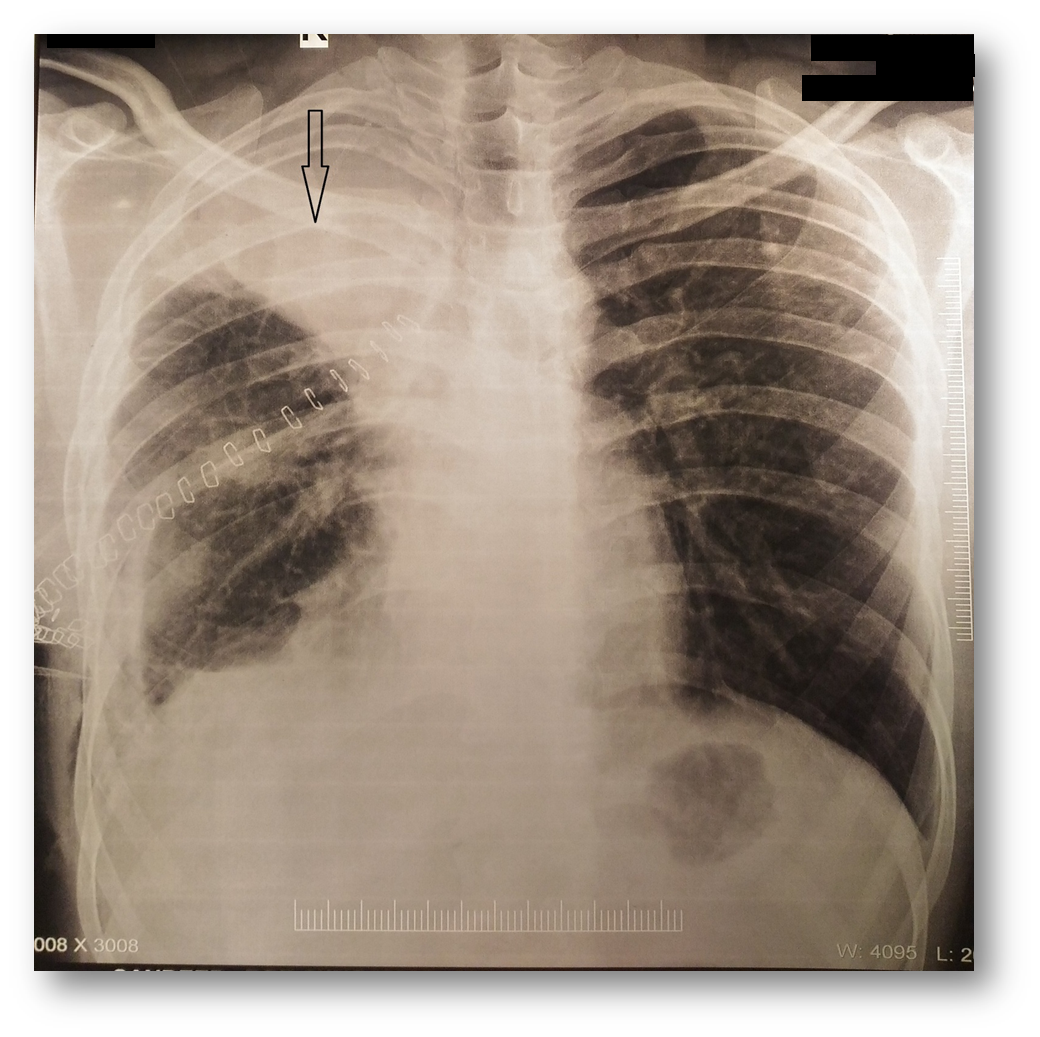
Figure 1. Chest x-ray showing opacity in the right upper zone.
Lung infarct is a rare complication of lobectomy. Commonly, postoperative infarct is due to pulmonary torsion and rarely due inadvertent ligation of the pulmonary artery or vein of the residual lobe. Here is a rare case of infarct of the residual upper lobe following a right upper lobectomy, presenting with opacity in the right upper zone, reported as “gossypiboma” by a radiologist.
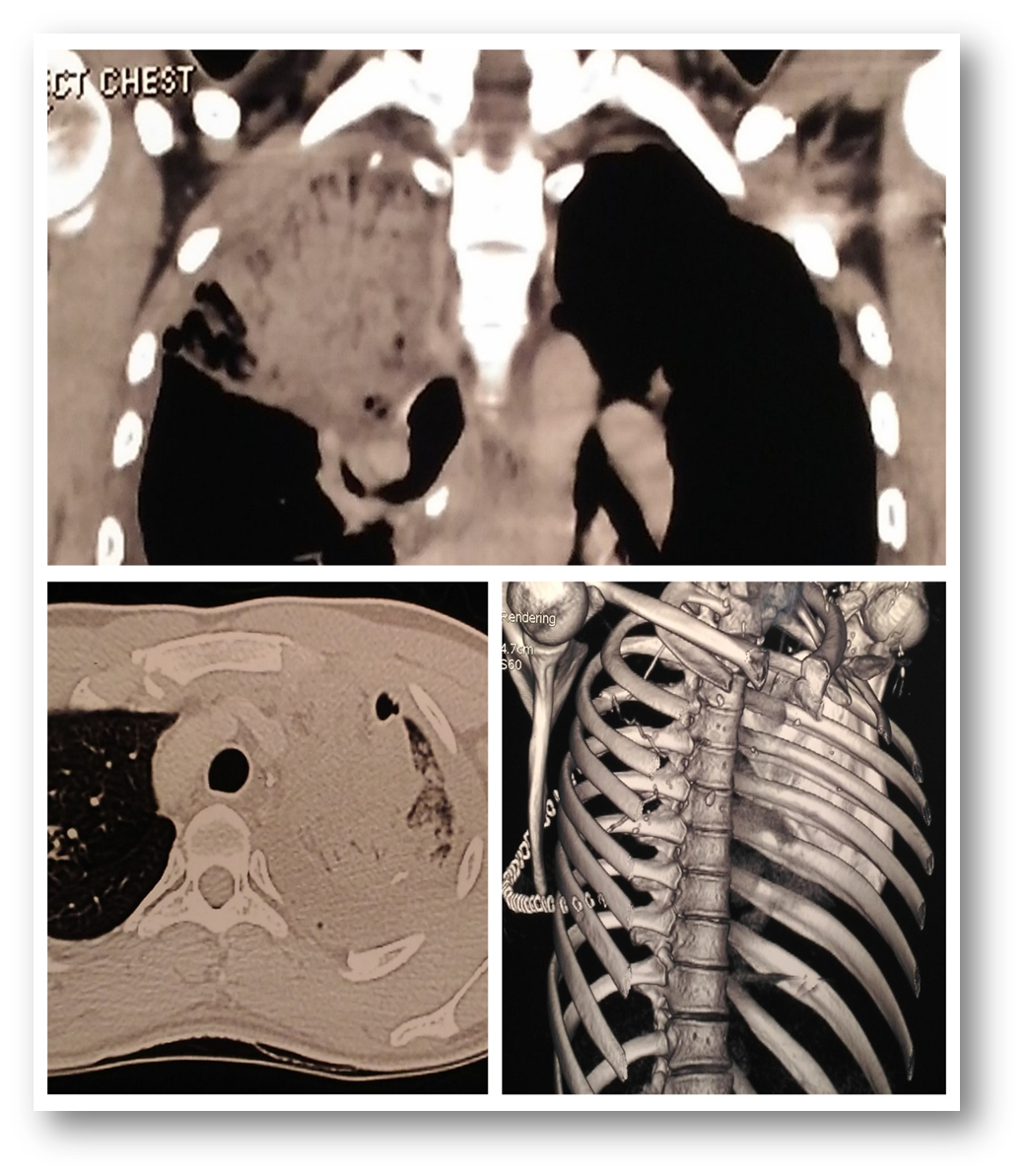
Figure 2. Contrast enhanced CT scan revealing an intracavity mass with air bubbles and a long radio-opaque marker.
A 21-year-old man in otherwise good health underwent a right upper lobectomy for aspergilloma. The surgery was uneventful. On the third postoperative day, he developed a fever and dull aching pain in his right chest. Plain x-ray revealed an opacity in the right upper zone (Figure 1). Contrast enhanced computed tomography (CT) scan revealed intracavity mass with air bubbles and a long radio-opaque marker, reported by the radiologist as a retained surgical sponge (gossypiboma) (Figure 2).
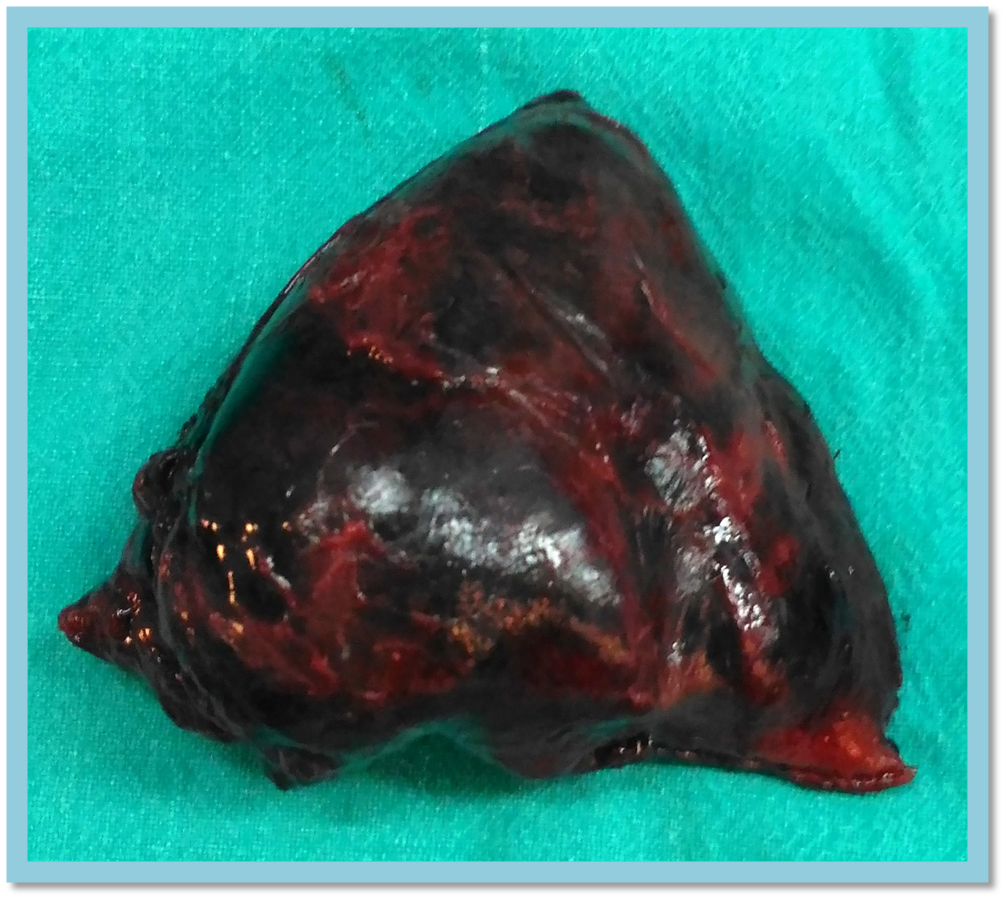
Figure 3. Infarcted residual upper lobe (excised specimen).
Based on the CT report, an immediate surgical re-exploration was done, and there was no retained sponge but an infarct of the residual right upper lobe was noted (Figures 3 and 4). It was found that the cause of infarct was a misinterpretation of the fissure during staple separation of the upper from the middle lobe after ligation of the upper lobe artery during right upper lobectomy, leading to infarct of residual devascularized lobe. The infarcted part was excised by wedge resection, and the patient recovered well postoperatively.
Discussion

Figure 4. Intraoperative image showing the healthy residual middle lobe in situ (arrow).
The authors’ case highlights the importance of keeping rare complications of surgery in mind. Careful and appropriate attention to the techniques of surgery is needed to prevent postoperative complications.
References
- Parissis H, Booth K, Al-Alao B. A case of focal lung infarction following right upper lobectomy in case of undeveloped lung fissure. Gen Thorac Cardiovasc Surg. 2015;63(9):522-525.
- Liebow AA, Hales MR, Bloomer WE, Harrison W, Lindskog GE. Studies on the lung after ligation of the pulmonary artery: II. Anatomical changes. Am J Pathol. 1950;26(2):177-195.



