
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Transaortic Access for TAVR: A Novel Adaptation for Valve Implantation
Introduction
Transcatheter aortic valve replacement (TAVR) has emerged as a successful treatment for patients deemed unsuitable for open aortic valve replacement (1). Well-described TAVR access approaches such as transfemoral (TF), transapical (TA), transsubclavian, and transcarotid have been successful (2, 3, 4, 5). However, despite multiple approaches, some patient’s aortic anatomy necessitates alternate strategies. One of the alternate access options gaining momentum is the transaortic (TAo) approach. This method has been well-described and is associated with favorable outcomes (6). Even so, it is not always preferable, as some vascular conditions restrict TAo access, such as: aortic calcification, available distance between the exposed aorta and aortic annulus, and catheter/sheath mobility (7). Here, the authors describe the successful treatment of severe aortic stenosis in a patient whose aortic anatomy precluded the traditional TAo approach. The authors used a 10mm Dacron graft anastomosed end-to-side to provide adequate distance between the aortic annulus and the sheath insertion site. This adaptation made effective management of a severely stenosed aortic valve possible while avoiding a tortuous thoracic aorta. This adaptation could be considered a safe alternative when conventional access is unachievable and currently described TAo access is impeded.
Case Report
An 89-year-old female with hypertension, coronary artery disease, and severe symptomatic aortic stenosis manifested as multiple syncopal episodes, was referred to the authors’ institution for possible TAVR. The patient had no family medical history of cardiovascular disease. Echocardiogram revealed aortic valve mean (31 mmHg) and peak (54 mmHg) gradients, max velocity (4.1 m/s), aortic valve area (0.49 cm2), left ventricular hypertrophy (LVH) accompanied by inferior wall hypokenesis, and an ejection fraction (EF) of 45%. The patient’s frailty and high-risk STS score (predicted mortality of 6.7 and morbidity of 25.5) made her a good candidate for TAVR. Due to the patient’s peripheral cardiac anatomy, the multi-disciplinary heart team decided a TAo approach was the best option for the patient.
Preoperative computed tomography angiography (CTA) demonstrated a short, tortuous ascending aorta, which precluded adequate co-axial alignment of the sheath. To optimize deployment and minimize paravalvular leak, a side-graft off the ascending aorta was used as a conduit extension.
A right parasternal mini-thoracotomy was made. The second costocartilage was removed and the mammary artery was clipped and divided. Upon opening the pericardium, the mid and distal ascending aorta was exposed. The distance from the exposed aorta to the aortic annulus was short, less than the 7.5 cm needed for a 26 mm Sapien valve. A partial cross clamp was placed on the ascending aorta and a 10 mm Hemashield graft was anastomosed to the aortotomy, in an end-to-side fashion, to extend the distance between the aortic annulus and the sheath insertion site (Figures 1 & 2).
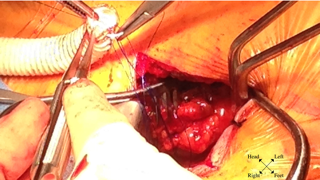
Figure 1: Performing 10 mm Hemashield graft end-to-side anastomosis to partially cross-clamped ascending aorta.
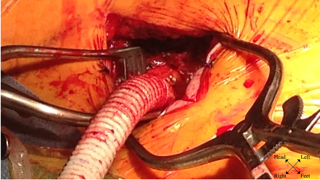
Figure 2: Completed side-graft extension off ascending aorta.

Figure 3: Ascendra delivery sheath secured to extended side-graft.
The graft was punctured with an 18 gauge needle followed by a 6F arterial sheath. A Kumpe catheter and straight wire were used to cross the aortic annulus. The straight wire was then exchanged for an Amplatz stiff wire, curved to fit the ventricle. After the Kumpe catheter was removed, an Ascendra delivery system was secured to the graft (Figure 3). Balloon valvuloplasty was then performed using a 23 mm balloon, followed by delivery of a 26 mm Sapien valve across the aortic annulus (Figure 4). Under rapid pacing, the valve was deployed. Transesophageal echocardiogram revealed a well-seated valve with trace perivalvular leakage. The Ascendra delivery system was then removed, and the graft was amputated proximal to the puncture site with clips and vascular stapler. There was no evidence of aortic dissection by TEE. The thoracotomy incision was closed in standard fashion. The patient remained intubated, in NSR, hemodynamically stable. She was discharged without complications, and was alive at one-year follow-up.

Figure 4: Sheath in side-graft (Arrow). Retrograde placement of percutaneous valve in aortic annulus prior to deployment.
Discussion
TAVR has rapidly become an efficacious treatment for high surgical risk patients with severe aortic stenosis (AS). Despite observed success, conventional TAVR approaches do not provide a therapeutic solution for all patients deemed unsuitable for open aortic valve replacement. Those patients with unfavorable femoral anatomy, previous cardiac surgery, and other contraindications to established TAVR approaches require new strategies, TAo, and, in some cases, modified approaches to successfully undergo transcatheter valve replacement.
This patient’s severe aortic tortuosity complicated a traditional TF approach. Although vessel diameter was adequate to accommodate the 26 mm Sapien valve and delivery system, an unfavorable thoracic aorta made the TF approach undesirable. Left ventricular hypertrophy has recently been considered a contraindication of the TA approach and its presence in the patient dissuaded the surgical team from an antegrade strategy (8). Lastly, the patient did not exhibit severe calcification of the ascending aorta, despite a heavily calcified aortic valve, which qualified her for a TAo approach.
Use of the graft permitted increased sheath mobility, balloon valvuloplasty, and subsequent valve deployment in spite of the patient’s adverse aortic anatomy. Regardless of the success of the TAo side-graft approach in this patient, there are putative disadvantages. Foremost, this procedure would not be appropriate for patients with a heavily calcified (porcelain) aorta, as this contraindication is known to complicate the traditional TAo approach and is not resolved by our modification (7). Additionally, using a side graft results in an aortic suture line and potential post-op bleeding.
Conclusion
The above-described procedure is a novel modification of the TAo approach when conventional TF, TA, and described TAo approaches are not feasible. A TAo approach employing a side graft on the abdominal aorta has been recently described, but to the authors’ knowledge, this is the first description of a successful adaptation of this similar procedure to the ascending aorta (9). This approach provided an adequate working annular to delivery system length. In conclusion, this modification addresses some of the critical issues that have previously inhibited the TAo approach, and may be used to re-qualify TAo access when initially contraindicated. This case demonstrates the adaptability of the TAo approach when a tortuous and/or a severely angulated aorta is present.
References
- Grube E., Sinning J.M. & Vahanian A. 2014. The Year in Cardiology 2013: valvular heart disease (focus on catheter-based interventions). Eur Heart J 35: 490-495.
- Himbert D, Roy D, Brecker S, et al: Tools and techniques: Transcatheter aortic valve implantation: Transfemoral approach. EuroIntervention 6:784-785, 2011.
- Walther T, Möllmann H, van Linden A, et al: Transcatheter aortic valve implantation transapical: Step by step. Semin Thorac Cardiovasc Surg 23:55- 61, 2011.
- Bruschi G, Fratto P, De Marco F, Oreglia J, Colombo P, Botta L, Cannata A, Moreo A, De Chiara B, Lullo F, Paino R, Martinelli L, Klugmann S. The trans-subclavian retrograde approach for transcatheter aortic valve replacement: Single- center experience. J Thorac Cardiovasc Surg 2010;140:911–915.
- Modine T, Sudre A, Delhaye C, Fayad G, Lemesle G, Collet F, Koussa M. Transcutaneous aortic valve implantation using the left carotid access: Feasibility and early clinical outcomes. Ann Thorac Surg 2012;93:1489–1494.
- Lardizabal J.A., O’Neill B.P., Desai H.V., Macon C.J., Rodriguez A.P., Martinez C.A., Alfonso C.E., Bilsker M.S., Carillo R.G., Cohen M.G., Heldman A.W., O’Neill W.W. & Williams D.B. 2013. The transaortic approach for transcatheter aortic valve replacement: initial clinical experience in the United States. J Am Coll Cardiol 61: 2341-2345.
- Bapat V. & Attia R. 2012. Transaortic Transcatheter Aortic Valve Implantation: Step-by- Step Guide. Semin Thorac Cardiovasc Surg 24: 206-211.
- Payne D.M., Rodes-Cabau J., Doyle D., De Larochelliere R., Villeneuve J. & Dumont E. 2012. Prominent septal hypertrophy: a contra-indication for transapical aortic valve implantation? J Card Surg 27: 309-311.
- Leucker T.M., Williams M.L. & Flaherty M.P. 2014. Transcatheter aortic valve replacement: a novel abdominal transaortic approach. Catheter Cardiovasc Interv 83: 670-675.



