
Introduction
Surgical stapling devices have been used in Thoracic surgery for over 20 years and have proven as reliable as suturing for the bronchus, pulmonary artery, pulmonary vein or lung parenchyma [1]. They have allowed for the widespread application of thoracoscopy to complex procedures within the chest. Until recently these staplers were hand fired requiring the hand of the surgeon or assistant to generate the force required to create a staple line while transecting the tissue. Advances in technology have allowed for the staple line to be created by the graduated and uniform application of force generated via a computer. The role of this technology in the arena of Thoracic surgery is still to be determined and whether it will positively impact on the way that operations are being performed is unknown. We describe the system, its working, our limited experience with it and a review of the current literature.
The System
SurgASSIST is the name that has been given to this new “Surgical Stapling Platform” by the manufacturer Power Medical Interventions which is based in Pennsylvania.
The components include
1. A Power Console (PC) which generates the power that fires the stapler and also the power that allows the remote control unit to control the flex shaft and the opening and closing of the stapler [Figure 1].
 |
| Figure 1 |
2. A Remote Control Unit (RCU) that allows manipulation of the flex shaft and the stapler itself within the thoracic cavity and the opening, closing and firing of the stapler [Figure 2].
 |
| Figure 2 |
3. A Flex Shaft (2.13 m) which is the cable that transmits the power generated from the computer to the stapler. This is two meters in length, flexible and can be manipulated within the thoracic cavity using the remote control or manually [Figure 3].
 |
| Figure 3 |
4. The Power Extender (40 cm) is a rigid linear handle that can be used to connect to the flex shaft when extra reach or rigidity is needed to manipulate the stapler within the thoracic cavity [Figure 4].
 |
| Figure 4 |
5. Digital Loading Units (DLUs) i.e. the stapler cartridges that both staple and cut tissue when fired. Both right angled and linear staplers can be used. The right angled staplers also cut allowing for a single application across a bronchus or a vascular structure [Figures 5a, 5b, 5c].
 |
 |
 |
| Figure 5a | Figure 5b | Figure 5c |
The types of DLUs currently available are:
- 75mm linear cutter with green-4.8mm, blue-3.5mm staple heights
- 55mm linear cutter with green-4.8mm, blue-3.5mm staple heights
- 45mm or 30mm Right angle cutter with green-4.8mm, blue-3.5mm, white-2.5mm (vascular) staple heights
- Circular stapler - 21mm (can be used per orally), 25mm, 29mm, 33mm.
The types of DLUs soon to be available are the linear cutters with a white (vascular) 2.5mm staple height.
The linear-cutting units are 15 mm in diameter; although they can be accommodated by a 15 mm port, the manufacturer suggests that they be used through a small accessory thoracotomy incision if VATS techniques are used.
Each DLU contains an electronic device that is programmed to activate a specific program in the microprocessor in the console.
When fired, the scalpel in the DLU cuts tissue distally first and proceeds proximally preventing tissue being displaced as is seen with conventional linear cutting staplers.
Use of the System
The Power console is a mobile unit that can be moved from OR to OR and plugs into an electrical power outlet. Both the Flex Shaft and the Remote Control Unit connect to the Power console. The Flex Shaft can be sterilized using gas / steam techniques and the end to which the DLU or Power Extender connects is brought up onto the operation field. The Remote Control Unit (RCU) can be controlled by a circulating nurse or using a sterile plastic cover for the unit, the surgeon. The DLU can be directly fixed to the Flex Shaft or to the Power Extender and this connection is simple with the DLU “clicking” into place. There is also feedback from the power console that indicates whether the DLU is properly loaded.
 |
| Figure 6: Open Stapler |
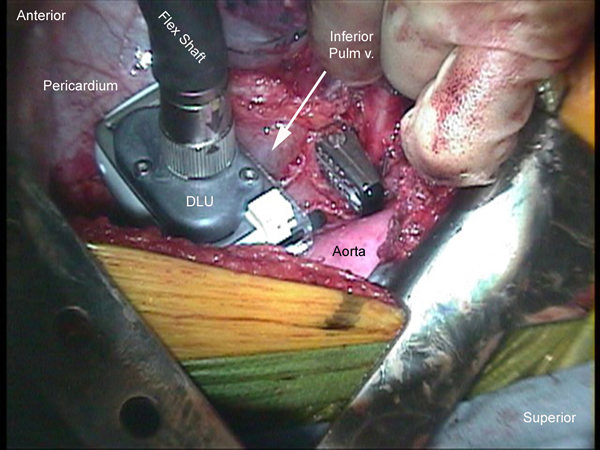
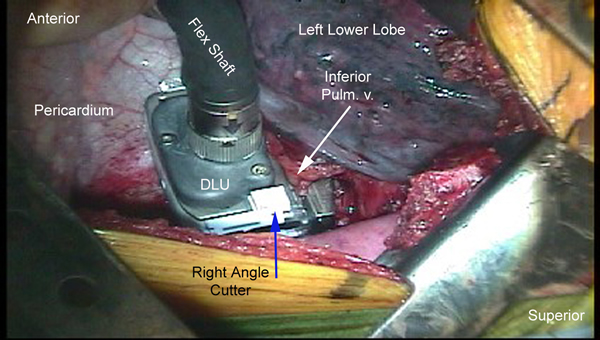
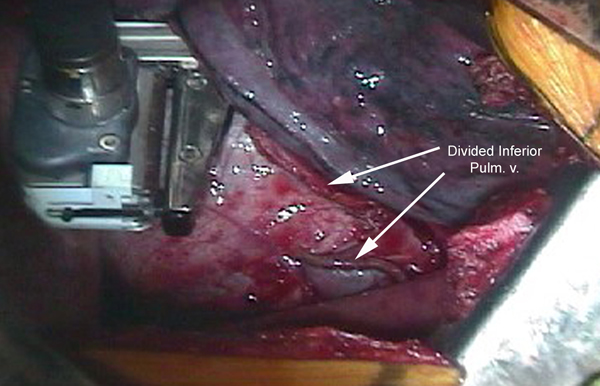
The DLU is then placed across the tissue to be stapled [Figure 6]. When using the right angled stapler it is sometimes necessary to position the DLU first and then connect it to the Flex Shaft. Once the DLU is positioned it is closed using the RCU. The computer in the PC then determines whether the DLU is appropriate for the tissue to be transected and it issues a “ready to fire” message on the liquid crystal display on the PC [Figure 7a]. If the PC senses that the tissue is too thick or there is too great a resistance, an “Out of Firing/Stapling Range” message is displayed and the DLU will not fire. An auditory prompt can also be heard for all of the steps involved with the “firing of the DLU”. This allows the surgeon to concentrate on the surgical field during the firing. The DLU is fired by deploying the “fire” button on the RCU. The staples are laid down and the tissue transected with the DLU opening once the firing is complete [Figure 7b].
 |
 |
| Figure 7a: Close Stapler | Figure 7b |
Pros:
- Easy to use, interactive system with feedback from PC. Voice prompts.
- Components work well together
- Remote computer generated power eliminates unnecessary force from site at the time of firing.
- Computer powered firing of stapler provides consistent staple formation.
- Flex shaft and Power extender allow versatility in the placement of the DLU.
- The linear cutters are reusable requiring a reload after each firing.
- Anvil closes from distal to proximal.
- The right angle DLU can staple and cut simultaneously.
- The DLU via the PC senses the thickness of tissue to be stapled and ensures that the appropriate staple height is selected.
Cons:
- Initial cost.
- The profile of the right angle cutter is sometimes too bulky to negotiate easily around branch pulmonary arteries.
- The right angle cutting stapler attaches to the shaft perpendicularly and not in line, making manipulation of this stapler around structures more difficult.
Cost
- Power console: $34,000
- Power Extender: $1500
- DLU- GIA: $300
- TA or Right angle cutter: $400
- Vascular: $400
- Circular stapler: $350
Results
The computer powered stapling system has been in use for the last 4 years [2]. It has been used primarily in general and gynecological surgery [1-6]. The application in Thoracic surgery has been recent and there are no large series documenting it’s use or benefit over conventional staplers [1].
Our preliminary experience at the Oregon Health Sciences University and Portland VA Medical center involved 30 firings of the stapler while performing open thoracic surgery. The stapler was used on the pulmonary vessels, the bronchus and the lung parenchyma with hemo- and pneumo-stasis that was comparable to conventional staplers. No misfiring of the stapler or malfunction of the system occurred during this time. No injuries to the stapled tissue or lung were encountered.
A recent series from France reports on the use of the system in 38 patients where the stapler was fired 26 times during open surgery and 12 times during VATS with no misfiring or malfunction [1]. For the use in VATS they experienced difficulty with the inability of the stapler to open widely and the excess flexibility of the flex shaft.
These issues have been now addressed by the inclusion of the Power extender and wider opening DLUs.
Discussion
More widespread experience with this system in thoracic surgery will likely determine the role for this new technology, which is currently in evolution [7]. Whether this technology facilitates minimally invasive or robotic thoracic surgery is another unanswered question. Experience with laparoscopy suggests that with continued improvements, the design of the system will evolve allowing easier performance of stapling during thoracoscopy [2].
The flexible shaft is currently difficult to manipulate both with open and thoracoscopic application. An instrument that combined features of both the flexible shaft and the power extender would improve considerably on the versatility of the system. A rigid shaft with a short remote-controlled flexible end allowing the DLU to reach the site of use easily and be placed around or across the tissue to be stapled would seem to make the most sense.
Slimming the profile of the right angle cutter to allow easier placement across vessels would be an improvement; making thoracoscopic lobectomy a technically simpler operation due to the ease of placing the stapler across the vessels.
The system is currently FDA-approved and as more thoracic surgical experience is gained and design advancements are made it will find its place in the armamentarium of the thoracic surgeon.
References
- Gossot D and Nana A. Computer-controlled stapling system for lung surgery. Ann Thorac Surg 2005;80:1898-901.
- Waage A, Gagner M, and Feng JJ. Early experience with computer-mediated flexible circular stapling technique for upper gastrointestinal anastomosis. Obes Surg 2003;13:88-94.
- Liem RK and Niloff PH. Clinical experience using the computerized digital stapling system in open gastric bypass surgery for morbid obesity. Obes Surg 2003;13:837-41.
- Balkhy HH, Chapman PD, and Arnsdorf SE. Minimally invasive atrial fibrillation ablation combined with a new technique for thoracoscopic stapling of the left atrial appendage: case report. Heart Surg Forum 2004;7:353-5.
- Martin ZL, Sweeney KJ, and Gorey TF. Peroral and transgastric esophageal anastomosis with flexible shaft remote-control stapler (SurgASSIST). Surg Laparosc Endosc Percutan Tech 2004;14:230-3.
- Waage A, Gagner M, Biertho L, et al. Comparison between open hand-sewn, laparoscopic stapled and laparoscopic computer-mediated, circular stapled gastro-jejunostomies in Roux-en-Y gastric bypass in the porcine model. Obes Surg 2005;15:782-7.
- Heitmiller RF. Invited commentary. Ann Thorac Surg 2005;80:1902.



