
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Intrathoracic Migration Of Breast Implant After Thoracoscopic Surgery
Breast implant complications after thoracic surgery are relatively rare. We present an unusual case of an intact implant migration into the pleural space after thoracoscopic surgery that was initially read as hemothorax on computed tomography of the chest.
Background
Breast augmentation with implants has been around since the 1960s and continues to gain popularity. As the recipients of breast implants grow in number and age, thoracic surgeons are more likely to encounter them in practice, and should therefore be prepared for possible challenges and complications of surgery.
Although iatrogenic rupture of breast implants is a recognized complication of thoracic surgery, breast implant complications as a whole are relatively rare [1-2]. Of all the complications, the migration of an intact implant into the thorax has only been reported twice previously, and only one case was related to open thoracic surgery [3-4]. We present what may the first report of implant migration into the pleural cavity after lung resection via minimally-invasive, Video-Assisted Thoracoscopic Surgery (VATS).
Case Presentation
Our patient was a 52 year old woman with a past history of uterine leiomyosarcoma treated with hysterectomy and chemotherapy in 2004. In 2010, she presented with non-specific cough symptoms and a chest x-ray demonstrating a left upper lobe mass. The diagnosis was an isolated 3.5 cm metastasis proven by needle-biopsy, with no evidence of disease elsewhere on Positron Emission Tomography (PET), Computed Tomography (CT), and brain Magnetic Resonance Imaging (MRI). Her cardiopulmonary function was normal and her past medical history was notable for breast implants inserted over 25 years ago. Plans were made to proceed with VATS lung resection for metastectomy, and the patient was counseled regarding possible adverse events related to routine VATS surgery, including rupture of the breast implant.
At the time of surgery, the patient was placed in the usual right lateral decubitus position and a fourth intercostal space access incision (5 cm) was made lateral to the left breast. A 2 – 3 cm breach of the left breast implant capsule was noted, though the prosthesis itself was intact. A plastic wound protector was inserted in the access incision and a VATS lingulectomy was performed without further incident. At the end of the procedure, the implant capsule was repaired with a running polyglactin suture, and the access incision was copiously irrigated and skin closed as per routine. The patient had an uneventful hospital stay and was discharged in the morning of post-operative day three.
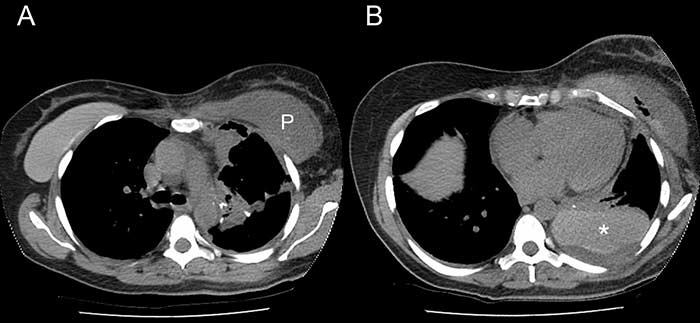
A. CT thorax showing the right implant in situ and the left implant capsule filled with pleural fluid (P).
B. The hyperdense left implant in the posterior pleural space (*) was misreported as hemothorax.
Open image in a new window
She returned to the emergency department twelve days later with pleuritic chest pain, nausea, and a low grade fever. A CT scan of the chest showed a high-density pleural effusion consistent with hemothorax. Since the patient was hemodynamically stable with no significant change in hemoglobin level, a pleural catheter was placed as the initial management. However, the effusion failed to resolve and further review of the imaging revealed that the left breast implant was no longer in the subpectoral position. What had been reported as blood in the pleural cavity was in fact the implant itself (Figure 1). The patient was brought to the operating room that day for VATS extraction of the implant and drainage of the pleural space. A Jackson-Pratt drain was inserted in the left breast implant capsule. She developed left mastitis post-operatively which was successfully treated with antibiotics and she was discharged five days later with follow-up with both thoracic surgery and plastic surgery.
In this case, the presence of a breast prosthesis was known prior to surgery and though the incisions were planned as for a routine VATS, a deliberate attempt was made to place the access incision lateral to the breast mound. Unfortunately, the implant capsule was still breached, which demonstrates the difficulty of predicting the edge of subpectoral breast implants. While it is unclear how the implant migrated into the pleural space after closure of the capsule, a major contributing factor is the fact that pericostal sutures are not typically used to close VATS access incisions, thus leaving a gap where intercostal muscles are divided. The pressure exerted by the left pectoralis muscle onto the implant may have been sufficient to disrupt the capsular repair and force the implant through the unclosed intercostal access incision. Since pericostal sutures cannot be used to obliterate the opened intercostal space, a possible alternative would be to use a mesh patch over the access incision instead.
Conclusions
We do not consider the presence of breast implants to be a contraindication to major VATS lung resection. We ensure that patients are well informed of the potential risk of implant-related complications. While plastic surgeons frequently close breast capsule incisions with simple running sutures in capsulotomy procedures, the presence of intercostal incisions in thoracic surgery opens the door to intrathoracic complications.
References
- Andersen B, Hawtof D, Alani H, Kapetansky D. The diagnosis of ruptured breast implants. Plast Reconstr Surg 1989;84:903-7.
- Rice DC, Agasthian T, Clay RP, Deschamps C. Silicone thorax: a complication of tube thoracostomy in the presence of mammary implants. Ann Thorac Surg 1995;60:1417-9.
- Chen ZY, Wang ZG, Kuang RX, Wang BT, Su YP. Implant found in thoracic cavity after breast augmentation. Plast Reconstr Surg 2005;116:1826-27.
- Mehta AM, Bard MPL, van Straten A, van Beijeren I, Rijna H. Intrathoracic migration of a breast prosthesis after thoracotomy. J Thorac Cardiovasc Surg 2008;135:206-7.



