
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Electromagnetic Guidance for Transbronchial Biopsy of Peripheral Lung Lesions: Navigational Bronchoscopy
Introduction

Figure 1: The Sahara S-1100 Deknatel drainage system with the 7 chamber air leak meter.
Although air leaks remain the most common complication after pulmonary resection, they have received little scientific study until recently. Despite the development and adoption of a classification system for air leaks [1, 2] and several recent prospective randomized studies that have evaluated different chest tube settings to best treat them [1, 3, 4] physicians are limited by the available technology that measures the air leak. Only the most sophisticated drainage systems for chest tubes have an air leak meter (Figure 1). Yet, despite the dramatic advance that the air leak meter has provided in the management of patients with leaks, the presence or absence of a leak still has subjective overtones and has not been completely quantified. For example, it is not uncommon for physicians to ask one another as they stare at an air leak chamber, "Was there really a bubble on that breath, was there really a leak, or was it just a momentum leak and the clearing of air with the first cough?" Often one experienced observer at the bedside will report a leak while another disagrees. Given the trend in the third millennium towards digitalization in many facets of life and especially in science, it is no surprise that several companies have applied digital technology to objectively measure the size of an air leak out a chest tube. Recently, Millicore, a Swedish company, developed the world’s first FDA approved digital air leak measurement system. It is currently available for sale in Europe and the United States. Other digital chest tube drainage systems are on the way.
Technology
The Digivent is a new pleural drainage system (Figure 2). It has a tear-shaped device called the controller unit. This device represents the “brains” of the Digivent. The size of the air leak in ml/breath is displayed on the controller unit. In addition, the nurse or physician is also able to see the average size of the leak over the past 1 hour, 3 hours or 6 hours. This allows one to assess how the leak is healing and the efficacy of the current chest tube setting. For instance, applying more suction to the chest tube will almost immediately increase the size of the air leak on the controller unit, but sometimes that may improve pleural–pleural apposition and help in the sealing of the air leak. Moreover, the controller unit also measures the maximum and minimal pleural pressures during the respiratory cycle (Figure 3). We have found that, as the two curves start to approach one another, the patient’s air leak is healing. This information affords one the ability to assess the optimal chest tube setting for each patient. The difference suction may have compared to water seal is readily displayed and the optimal amount of suction can be ascertained.
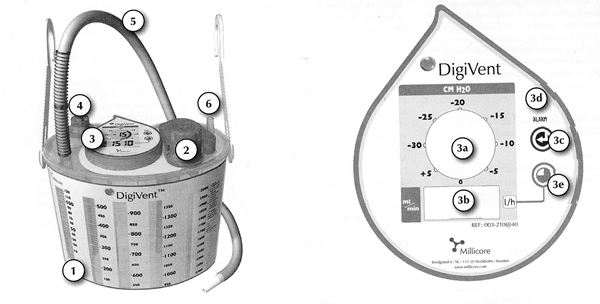
Figure 2: The Digivent apparatus and its controller unit (1- collection chamber, 2-suction dial, 3-controller unit, 3a-indicates amount of suction applied, 3b-digital air leak read out (ml/min), 3c-return, 3d-hi/low pressure alarm, 3e-accumulation button l/h, 4-pressure relief valve, 5-patient tube, 6-suction tubing port).
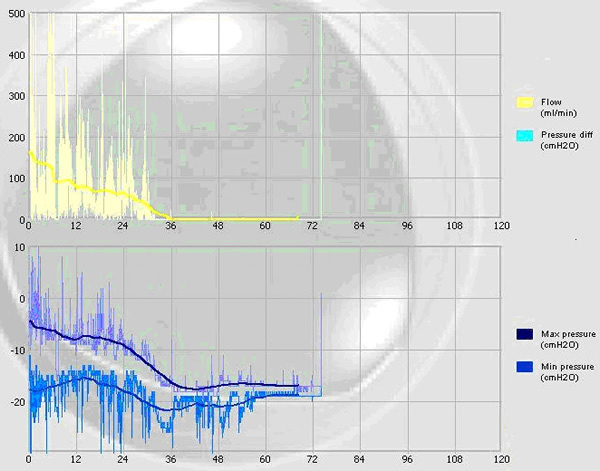
Figure 3: Tracings of the maximal and minimal pleural pressures in a typical patient with an air leak as measured by the Digivent. Note as the maximum and minimum pressures approach one another the leak is resolving.
Clinical Use
In a prospective randomized study, we evaluated the Digivent and compared it to the drainage system that we currently employ and which has been studied the most extensively, the Sahara Pleur-evac. We found that the Digivent detected an air-leak in several patients who had equivocal air leak exams on the Sahara system. The pleural space pressure curves suggested a pneumothorax which was confirmed by a chest x-ray in three patients. Patients randomized to the Digivent had their chest tubes removed sooner (p=0.03) and also enjoyed a shorter hospital length of stay (p=0.05) because of the confirmation of the absence of air leaks and because we could more objectively decide on optimal chest tube settings and removal. The average time for air-leak assessment at the bedside was significantly less for the Digivent and physician, nurse and patient satisfaction was higher with the Digivent despite the initial learning curve that all new devices require.
Our preliminary findings indicate that water seal is better for most leaks but not all. Importantly, the pressure curves may also be able to predict when a pneumothorax has occurred or is occurring, although more data is required to fully sort out this issue. Theoretically, this device could then prevent the time, expense and patient discomfort associated with chest x-rays that many physicians perform daily in patients with a chest tube in place.
Conclusions
The Digivent is a new digital device that allows physicians to quantify the size of air leaks objectively. It almost eliminates the subjectivity to air leaks and may allow for more uniform chest tube management and thereby shorten the length of stay as well as the number of patients that are discharged home with their chest tube in the pleural space. The Digivent is more accurate and easier to use than the current air leak system. Finally, this device generates air leak curves that may predict when a patient is developing a pneumothorax and this may help avoid the need for a chest radiograph. Larger, multi-institutionally studies are needed to corroborate our findings and to generate more data on the interpretation of the data that is gleaned from the Digivent. Finally, the cost effectiveness of this device must be determined to fully identify its role in the care of patients who undergo pulmonary resection.
References
- Cerfolio RJ, Bass C, Katholi CR. Prospective randomized trial compares suction versus water seal for air leaks. Ann Thorac Surg 2001;71:1613-7.
- Cerfolio RJ. Advances in thoracostomy tube management. Surg Clin N Am 2002;82:833-48.
- Marshall MB, Deeb ME, Bleier JI, et al. Suction vs water seal after pulmonary resection: a randomized prospective study. Chest 2002;121:831-5.
- Brunelli A, Monteverde M, Borri A, et al. Comparison of water seal and suction after pulmonary lobectomy: a prospective, randomized trial. Ann Thorac Surg 2004;77:1932-7.



