
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Wedge Resection of Solitary Pulmonary Nodules Through Uniportal VATS
Patient Selection
Patients with lung lesions located in the outer third of the lung are suitable candidates for uniportal VATS resection. When used for the diagnosis of interstitial lung diseases or in the treatment of primary pneumothorax, the procedure is facilitated by the immediate identification of the area to be resected. Pulmonary nodules can be easily identified, without the need for marking, when they are located at the fissure or at the lobar edges. The addition of fluoroscopically-guided hookwire, injection of methylene blue, or ultrasonic identification allows for resection of more deeply situated nodules that are otherwise not immediately detectable. Exclusion criteria are the ones valid for the standard VATS approach, i.e. centrally located lesions, previous thoracotomy, extensive lung consolidation, and inability to achieve one lung ventilation. Since the existence of a learning curve has to be acknowledged, there must be no hesitation to convert to a two- or three-port VATS approach in the event of technical difficulty. In addition, a thoracotomy tray must be immediately available in theater.
Operative Steps
The procedure is carried out under general anesthesia with a double lumen endotracheal tube in place and with the patient in a lateral decubitus position. A single 2 -2.5 cm incision is made taking care to face the lesion at a suitable distance to avoid mutual interference of the VATS instrumentation [1]. For a lesion located in the apical segment of the lower lobe or in the posterior segment of the upper lobe, an incision in the safety triangle is preferable (triangle in the axilla defined by the border of the pectoralis major muscle, anteriorly, the latissimus dorsi, posteriorly, and, a horizontal line at the level of the fourth intercostal space). For lesions in the middle lobe, the lingula or the anterior segments of the upper and lower lobes, an incision in the 5th intercostal space along the scapular line is recommended. For lesions located at the apex of the lung, an incision at the level of the 5th intercostal space in the posterior axillary line is used.
Gentle spreading with a Roberts clamp is used to enter the chest superior to the immediately underlying rib, in a fashion similar to placement of a chest drain. Since a 3 or 5 mm videothoracoscope and the operative instruments need to be introduced through the same port, the incision is gauged to fit the surgeon’s index finger (Video 1 below). The general geometric rationale behind this approach is summarized in a previous report [1].
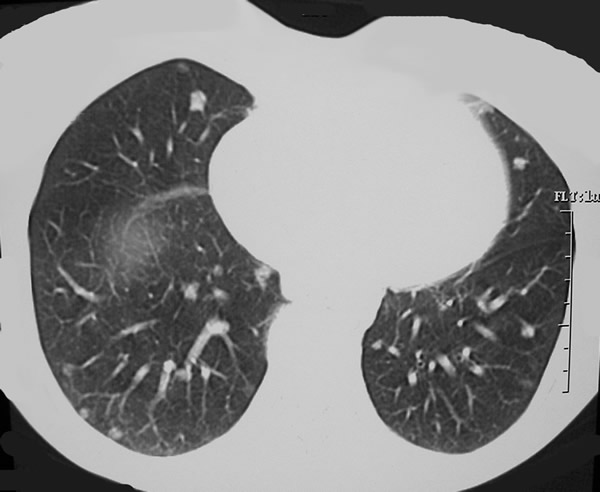
Figure 1. Chest CT showing multiple nodules in both lungs. Preoperative identification of the most suitable nodules to be resected by uniportal VATS is of paramount importance to the success of the procedure.
In the illustrative case (Figure 1), the target lesion is identified in the right middle lobe (Video 2 below). A roticulating endograsper is introduced parallel to the videothoracoscope with the port sleeve retracted along the stem and held in place by the same hand holding the scope. The roticulating arm of the grasper is displayed so that the grasper stem is confined at one corner of the incision while the grasping end of the arm is suspending the nodule cranially (Video 3 below). At this time, the assistant is holding the videothoracoscope by standing aside the surgeon. A roticulating endostapler is introduced with the roticulating edge already rotated upward with the thinner component on the right hand side. This is to facilitate the introduction of the endostapler in a narrow space by holding the stem of the instrument as a pen and gently sliding the endostapler, parallel to the videothoracoscope, as “a mediastinoscope under the pretracheal fascia”. The endostapler is inserted deeply into the chest in order to position the fulcrum inside the cavity thus allowing for jaws opening. At this point, the thinner anvil is immediately recognizable. At all times the insertion of the instruments inside the chest be should be observed using the thoracoscope. The surgeon holds both the endograsper and the stapler so that the stapler is positioned caudally to the lesion and the grasper gently positions the parenchyma between the jaws. At this point, the jaws are closed and the inclusion of the nodule in the specimen is visually confirmed. The endostapler is then fired, the jaws are opened, and the instrument is removed from the chest following the reverse sequence of movements that were used for the insertion. Multiple firings of the endostapler may be needed in order to fully detach the parenchyma from the lung (Video 4 below). Endoscissors can be also used to cut small bridges of tissues. Once the lesion is successfully wedge resected, an endobag, can be used to remove the specimen (Video 5 below). After hemostasis has been secured, a chest drain is inserted through the same port site.
Preference Card
- 3 or 5 mm videothoracoscope (0° and 30°)
- Roticulating graspers and endostaplers
- Endoshears and endobags
Tips & Pitfalls
- Solitary pulmonary nodules are by definition lesions measuring less than 3 cm located in the outer third of the lung: uniportal VATS wedge resection must be reserved to these pulmonary lesions.
- Preoperatively, the choice of the location for the only port site should be based on a careful evaluation of chest CT. The need for an anterior placement of the port because of fear of chest drain kinking should not be overemphasized. The patient can be instructed to lie slightly (45°) on one side. In some circumstances, placement of a chest drain at the end of the procedure can be avoided.
- Make sure that a thoracotomy tray is always opened and ready. No hesitation to convert to two or three port incision, if not to a limited thoracotomy, should interfere with the safe performance of the operation.
- Hemostasis of the single port at the time of its creation is of paramount importance to save time and frustration later when the telescope lens needs to be repeatedly wiped from drops of blood running down from the chest wall onto the videothoracoscope.
- Take full advantage of the laterality offered by the port incision; every effort should be made to avoid leverage on the intercostal bundles running along the inferior border of the overlying rib.
- Bear in mind that, to avoid interference of the instrumentation inside the chest, there must be a certain distance from the lesion.
- Always remove the trocar sleeve along the thoracoscope stem and hold it in place outside of the incision in order to save room for the operative instruments.
Results
Recently, uniportal VATS wedge resections have been suggested as a potential alternative to the traditional three-port VATS approach in the diagnosis and treatment of several pulmonary conditions[1-3]. A demonstrated advantage of uniportal VATS is represented by a decreased incidence of postoperative pain and paresthesia, possibly related to the reduced number of ports used during the procedure [4].
Similar to three-port VATS, the major caveat of uniportal VATS wedge resections for SPNs lies in the need to identify by preoperative marking those lesions which may not be readily visible in the absence of the potential for digital exploration. In the future, the availability of ultrasound probes to be used thoracoscopically and the resort to localization with technetium may enhance the discrimination of peripheral nodules [5].
The instrumentation used in uniportal VATS may be more expensive, but the extra cost might be offset by a reduction of hospital stay [1]. In this setting, some surgeons have found that there mat be no need for a chest drain following wedge resection of the lung [6]. The use of high loco-regional analgesia in awake patients undergoing uniportal VATS wedge resections of the lung will probably further decrease costs and hospital stay and expand the indications for utilization of this technique in an outpatient setting [7].
References
- Rocco G, Martin-Ucar A, Passera E. Uniportal wedge pulmonary resections. Ann Thorac Surg 2004;77:726-8.
- Rocco G, Khalil M, Jutley R. Uniportal VATS wedge lung biopsy in the diagnosis of interstitial lung disease. J Thorac Cardiovasc Surg 2005;129:947-948.
- Ng CSH, Rocco G, Yim APC. Video-assisted thoracoscopic surgery (VATS) pleurodesis for pneumothorax. MMCTS 2005;doi:10.1510/mmcts.2004.000349
- Jutley RS, Khalil MW, Rocco G. Uniportal vs standard three-port VATS technique for spontaneous pneumothorax: comparison of post-operative pain and residual paraesthesia. Eur J Cardio-Thorac Surg 2005;28:43-6.
- Daniel TM, Altes TA, Rehm PK, et al.
A novel technique for localization and excisional biopsy of small or ill-defined pulmonary lesions. Ann Thorac Surg 2004;77:1756–1762. - Watanabe A, Watanabe T, Ohsawa H, et al.
Avoiding chest tube placement after video-assisted thoracoscopic wedge resection of the lung. Eur J Cardio-Thorac Surg 2004;25:872-6. - Pompeo E, Mineo D, Rogliani P, Sabato AF, Mineo TC. Feasibility and results of awake thoracoscopic resection of solitary pulmonary nodules. Ann Thorac Surg 2004;78:1761-1768.
Video 1
Video 2
Video 3
Video 4
Video 5



